| |
|
CANCERS IN HIV-INFECTED PATIENTS
|
| |
| |
These 2 studies were reported at ICAAC (Dec 2001). The first study from Nunez
in Spain reports that non-hodgkin (NHL) and Hodgkin lymphoma were associated
with lower CD4 counts even if people were on HAART. In the 2nd study
discussed below, researchers looked at HIV+ patients in the Veteran's
Administration system. They found HIV+ patients were more likely to have
cancers than HIV-negative patients in the VA. The authors of the second study
suggest lifestyle may play a contributing factor. For example, HIV+ patients
may be more likely to be former IVDUs, etc.
I don't know of any studies exploring the possibility that taking many drugs
for HIV and related complicaions may play a contributing role in increasing
risk for developing a cancer. So I don't think we have any research data on
that possibility. This is purely speculative on my part. Persons with HIV
tend to be more sedentary, perhaps smoke cigarettes more, is diet worse in
terms of fats?, do they take more adjunctive drug therapy & does this
contribute to perhaps increasing cancer risk?.....Or, is HIV and/or a low CD4
count a contributing factor......How does the risk for cancer in HIV relate
to "when to begin HIV therapy". In addition to the many real considerations
discussed at length relating to the question of when to begin therapy, is
delaying initiation of HAART until CD4s are low, perhaps <350, or perhaps
when viral load is >50,000, contribute to the risk for developing cancer. We
do not have answers to these questions.
Trends in the Occurrence of Cancer in HIV-Infected Patients in the Era of
Highly Active Antiretroviral Therapy (HAART). Abstract I-248
M. NUNEZ, M.E. VALENCIA, I. JIMENEZ-NACHER, L. MARTIN-CARBONERO, R.
RODRIGUEZ-ROSADO, V. SORIANO, J. GONZALEZ-LAHOZ
Instituto de Salud Carlos III, Madrid, Spain
Background: The introduction of HAART has led to dramatic reductions in the
incidence of some AIDS-related tumors, while the incidence of other
malignancies seems to remain unchanged or to be on the rise.
Methods: Patients with a diagnosis of cancer were retrospectively identified
among all HIV+ subjects seen at a reference HIV-Hospital between 1996 and
2000. The cumulated incidence of malignancies was calculated for every year:
number of tumors diagnosed/number of HIV+ subjects attended in a certain
year. Age, HIV risk factor, CD4+ and use of HAART were recorded.
Results: 75 malignancies were identified. The HIV factor of patients was as
follows: IVDU 27 (40%), homosex. 28 (41%), heterosex. 13 (19%). The
male/female ratio was 48/21. Mean (range) age and CD4 counts were 39 (23-64)
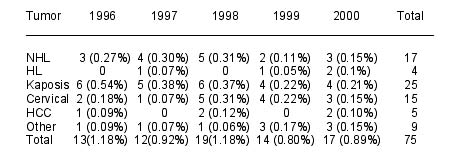
and 323 (7-1111) respectively. Table shows the number of cases and cumulate
incidence (in brackets) by year of diagnosis and type of tumor. Non-Hodgkin
(NHL) and Hodgkin (HL) lymphomas were significantly associated with lower CD4
counts regardless the use of HAART (p=0.02). Age was higher for subjects with
hepatocarcinoma (HCC) (p=0.01).
|
|
 |
| |
Conclusions: Malignancies are gaining importance over opportunistic
infections among the HIV+ population during the HAART era. Most tumors were
diagnosed in patients with relatively preserved immunity and predominantly in
prior IVDU or homosexual men. While the incidence of KS and NLH is
decreasing, HCC and other non-AIDS defining tumors are expected to become
more frequent with the increase in life span of HIV+ patients.
Total Cancer Incidence Among HIV+ Veterans Relative to the General
Population.
Abstract: I-249
K. MCGINNIS, A. JUSTICE, J. WAGNER
VA Pittsburgh Center for Health Services Research, Pittsburgh, PA
Background: As people with HIV are living longer on treatment, there has been
growing concern that they may be at substantially increased risk for cancer.
To examine current cancer patterns in HIV+ persons, we compared cancer
incidence among a cohort of HIV+ veterans enrolled in the Veterans with
HIV/AIDS Cohort Study (VACS) to cancer incidence in the general population
using the Surveillance, Epidemiology, and End Results (SEER) Cancer Incidence
Public-Use Database, 1973-1997.
Methods: The 868 HIV+ male veterans were used in this initial analysis. Using
ICD-9 diagnosis codes assigned in the Veterans Affairs electronic medical
records we calculated observed cancer incidence rates (IRs) for these HIV+
veterans from January 1998 to December 1999. Using 1996 and 1997 SEER data,
the most recent two-year interval available, age-adjusted cancer IRS were
calculated for males ages 25-84. Poisson regression was used to calculate
age-adjusted VACS to SEER rate ratios for specific and total cancers with 95%
confidence intervals.
Results: Oral cavity and pharnyx (oral), digestive system, respiratory
system, skin, male genital system, ill-defined, and total cancers were
compared. Each of these age-adjusted cancer IRS occurred among HIV+ veterans
in statistically significant excess over the general population: oral (RR =
9.41; CI = 3.5-25.1; p-value <.001), digestive (RR = 2.63; CI = 1.1-6.3;
p-value = 0.030), respiratory (RR = 3.1; CI = 1.3-7.5; p-value = 0.011), skin
(RR = 13.2; CI = 7.3-23.9; p-value < 0.001), male genital (RR = 2.9; CI =
1.5-5.8; p-value = 0.002), ill-defined (RR = 30.8; CI = 13.8-68.6; p-value
<.001), and total (RR = 4.8; CI = 3.6-6.4; p-value <0.001).
Conclusions: For all categories compared age-adjusted cancer rates were
elevated among HIV+ veterans compared to the general population. While some
of this may be explained by differences in lifestyle and other exposures, the
magnitude of risk suggests that HIV or its treatment may put individuals at
greater risk for subsequent cancer.
|
|
| |
| |
|
|
|