 |
|
|
| |
Early HAART Associated with Improved Outcomes & Fewer Toxicities
|
| |
| |
Reported by Jules Levin
13th CROI
Denver, Feb 5-8, 2006
"Estimating the Optimum CD4 Threshold for Starting HAART in ART-naive HIV-infected Individuals"
Starting HAART when CD4s are 350-500 was safer regarding clinical progression than starting when CD4s were 200-350
Jonathan Sterne*1, M May1, D Costagliola2, M Egger3, R Hogg4, A D'Arminio Monforte5, G Chene6, M Gill7, F De Wolf8, S Cole9, and ART Cohort Collaboration
1Univ of Bristol, UK; 2INSERM U720, Hosp Pitie-Salpetriere, Paris, France; 3Inst of Social and Preventive Med, Univ of Berne, Switzerland; 4Univ of British Columbia, Vancouver, Canada; 5Inst of Infectious and Tropical Diseases, Univ of Milan, Italy; 6Inst de Sante Publ, Univ Victor Segalen, Bordeaux, France; 7Southern Alberta HIV Clin, Calgary, Canada; 8HIV Monitoring Fndn, Academic Med Ctr, Univ of Amsterdam, The Netherlands; and 9Johns Hopkins Univ, Bloomberg Sch of Publ Hlth, Baltimore, MD, US
ABSTRACT
Background: The question of exactly when HAART should be started is unresolved. Previous analyses that compared disease progression according to immunodeficiency at HAART initiation may have been biased as they generally ignored the lead time (the time it takes for patients starting later to reach the lower CD4 count) and unseen events that occur in the deferred group. In particular, patients who deferred treatment, but progressed to AIDS or died while untreated are not represented in analyses comparing rates of progression to AIDS in those starting HAART at different CD4 counts.
Methods: We estimated hazard ratios (HR) comparing individuals starting HAART when CD4 count fell between 500 and 351 cells/mL with those starting between 350 and 201 cells/mL; we also compared those starting between 350 and 201 cells/mL with those starting <200 cells/mL.
We estimated the time to cross the CD4 thresholds and the time to AIDS using data from the Multicenter AIDS Cohort Study (MACS) during the pre-HAART era (1989-1995). Data from 10,885 individuals in the ART Cohort Collaboration (ART-CC) who were AIDS-free and ART-naive at HAART initiation were used to estimate rates of progression to AIDS after HAART initiation. For individuals starting HAART below the CD4 threshold, lead time was imputed 25 times by randomly sampling from the pre-HAART-era distribution. Data on "unseen" individuals progressing from the upper CD4 threshold to AIDS in the absence of therapy were also imputed 25 times. Standard methods for combining results from multiple imputed datasets were used to derive overall HR and 95% CI.
Results:
CD4 count at initiation of therapy was <200, 201 to 350, and 351 to 500 cells/mL for 40%, 37%, and 23%, respectively. Median length of follow up was 2.7 years (IQR 1.2 to 4.4 years).
There was clear evidence that individuals starting <200 had higher progression rates than those starting between 201 and 350 cells/mL (HR for AIDS 3.30, 95%CI 2.51 to 4.33) after accounting for lead time and unseen events. Comparing individuals starting at 201 to 350 with those starting at 351 to 500 cells/mL, the corresponding HR was 1.46 (95%CI 0.96 to 2.21).
Conclusions: Our results provide evidence that over several years, AIDS rates are lower in individuals who initiate HAART at higher CD4 counts. However, these results must be discounted for possible disadvantages of early initiation of therapy, including adverse effects of HAART and potential exhaustion of future treatment options.
"Early, Uninterrupted ART Is Associated with Improved Outcomes and Fewer Toxicities in the HIV Outpatient Study (HOPS)"
Kenneth Lichtenstein*1, C Armon2, K Buchacz3, A Moorman3, K Wood2, J Brooks3, and HIV Outpatient Study
1Univ of Colorado Hlth Sci Ctr, Denver, US; 2Cerner Corp, Vienna, VA, US; and 3CDC, Atlanta, GA, US
Background: Concern about HAART-related toxicities have led to guidelines that advocate delayed initiation of therapy. Using the HOPS cohort, we analyzed the response to HAART and the incidence of selected toxicities by pre-HAART CD4 cell count (pHCD4) and by time on HAART once initiated.
Methods: We analyzed a prospective, dynamic cohort of >7800 patients followed since 1993. We stratified patients by pHCD4 (0 to 49, 50 to 199, 200 to 349, 350 to 499, and >500 cells/mm3) and by time on HAART after initiation (took ≥95% of the time vs <95% of the time) and before development of toxicities. We used c2 and logistic regression analyses to assess risks for developing three toxicities: renal insufficiency, peripheral neuropathy, and lipoatrophy in the HAART era.
Results:
Of 2304 patients seen in HOPS clinics at least twice from 1996 to June 30, 2005, there were 124 with renal insufficiency, 278 with peripheral neuropathy, and 168 with lipoatrophy.
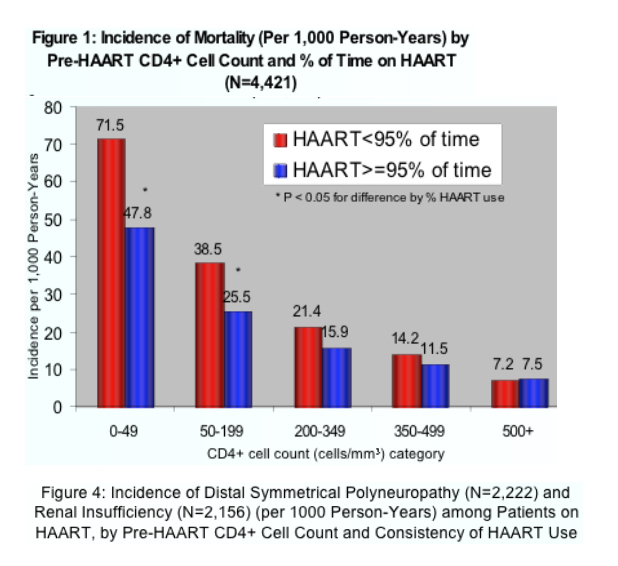
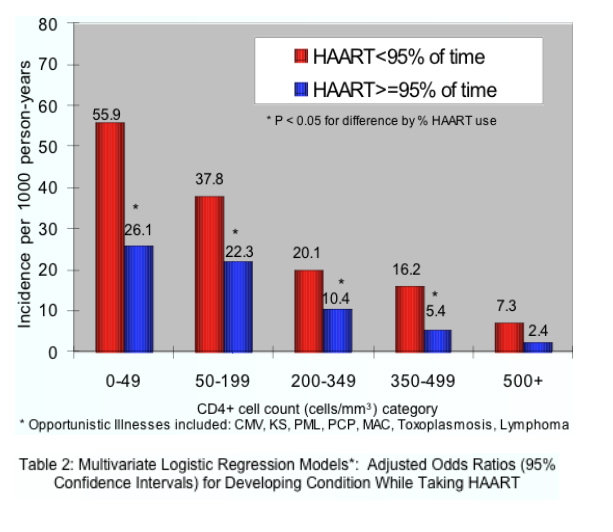
Approximately 31% of patients received HAART <95% time during follow-up. For each pHCD4R, after 8 years on HAART, CD4 count responses were higher (p <0.001) and the percentage of patients achieving viral loads <50 copies/mL greater (p <0.002) for the ≥95% group vs the <95% group. Incidence of death and of AIDS-defining illnesses decreased with higher pHCD4 (p <0.01) and at each pHCD4 was lower in the ≥95% group vs <95%.
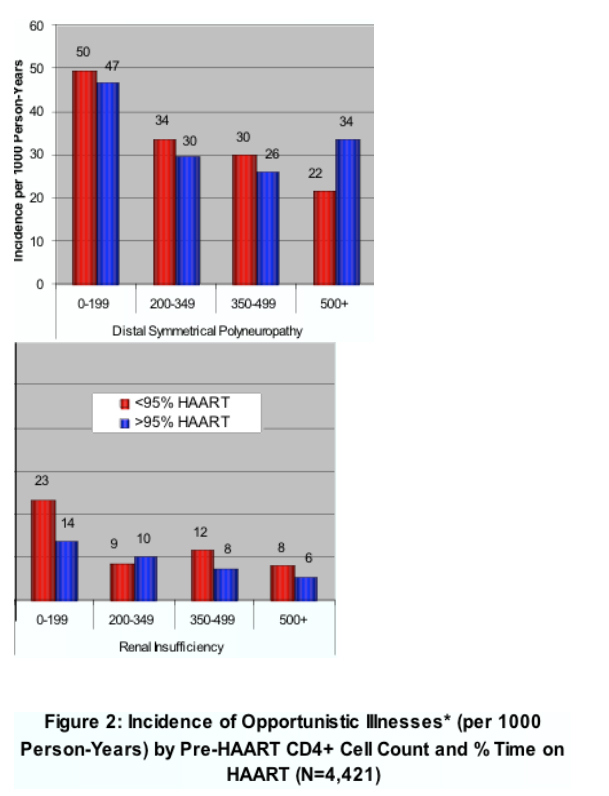
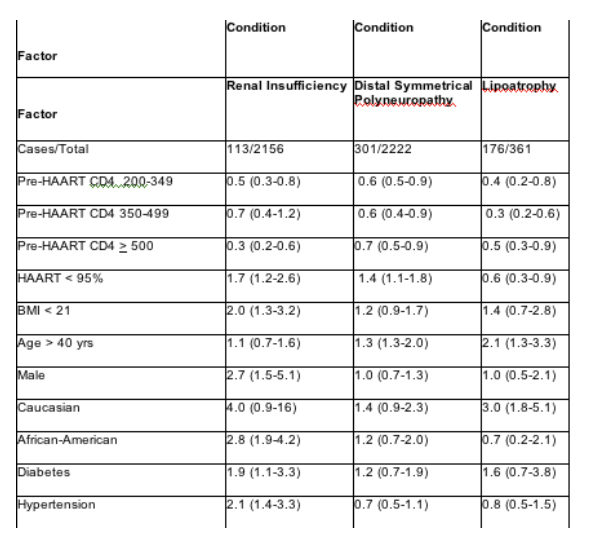
In multivariate analyses of demographic and clinical factors associated with incident toxicities, persons with higher pre-HAART CD4+ cell counts were consistently less likely to develop these toxicities (Table 2, see table below). In addition, persons who took HAART <95% of time were more likely to develop renal insufficiency and distal symmetrical polyneuropathy than persons who took HAART ≥95% of time; however, the reverse association was seen for lipoatrophy.
Univariate analyses found significantly decreased risk for renal insufficiency, peripheral neuropathy, and lipoatrophy among patients initiating HAART at higher pHCD4 and who remained on HAART ≥95% of the time.
In multivariate analyses, independent (p <0.05) risk factors for each outcome were as follows (adjusted odds ratio shown in parentheses):
for renal insufficiency, pHCD4 200 to 349 (0.6), 350 to -499 (0.4), >500 (0.3); <95% time on HAART (1.9); hypertension (2.1); African American race (1.6); body mass index <21 (1.9); ART-naive (2.9);
for peripheral neuropathy, pHCD4 200 to 349 (0.7), 350 to 499 (0.6), >500 (0.7); <95% time on HAART (1.5); age >40 years (1.3); stavudine 40 mg twice daily (1.8); any protease inhibitor (PI) (1.3); and for lipoatrophy, pHCD4 200 to 349 (0.5), pHCD4 350+ (0.4), age >40 years (1.8), white race (2.7), stavudine 40 mg twice daily (1.8), didanosine (1.6), tenofovir (0.6), any PI (2.1).
Conclusions: HOPS patients with higher pre-HAART CD4+ cell counts were less likely to develop renal insufficiency, peripheral neuropathy, and lipoatrophy in the HAART era, suggesting the benefit of earlier HAART treatment. Our findings also raise the possibility that use of HAART without interruptions may reduce the incidence of these complications.
|
|
| |
| |
|
|
|
|
|