 |
|
|
| |
Diagnosis and management of cognitive
disorders during successful HIV treatment
|
| |
| |
Reported by Jules Levin
EACS Nov 14 2009 Cologne Germany
From Jules:of note in this report the presenter Renaud Du Pasquier found from a study that 64% of patients who were NOT complaining of cognitive impairment had ANI (asymptomatic neuro-cognitive impairment) or (MND) mild neurocogbitive disorders.
This was in addition to those patients who were complaining of whom 8% had HIV-dementia and 52% had MND. In this study of 200 HIV+ individuals average age was 47, they had HIV for 14 yrs, undetectable HIV for 3-4 years, CD4 of 550-650, nadir CD4 of 160-185, 14-24% HCV+, and 27% had cognitive complaints. He suggests HAART with a high penetration score may improve cognitive impairment for many. Perhaps some damage due to HIV is irreparable. He suggests psychological testing in the clinic. He reviews similarities between alzheimer's and the effects of HIV on the brain, which has been the subject of other publications and discussions.
Renaud Du Pasquier
Neurology and Immunology
Lausanne, Switzerland

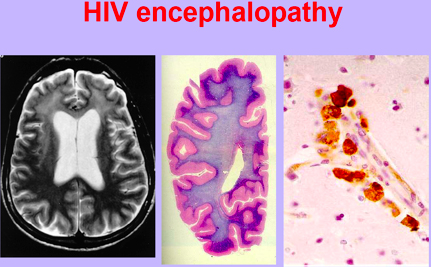
Beta-amyloid deposition in the frontal cortex of AD (a) and AIDS brains (b-d) detected by immunocytochemistry with the 4G8 monoclonal antibody (red staining). Compared to the classic beta-amyloid deposition in the AD brain predominantly as extracellular pl aques (a), in AIDS, beta-amyloid can be frequently found in the neuronal soma (c, and d, higher magnification) in addition to numerous plaques (b and c). Light microscopy, a-c (original magnification 20 X), d (60X).
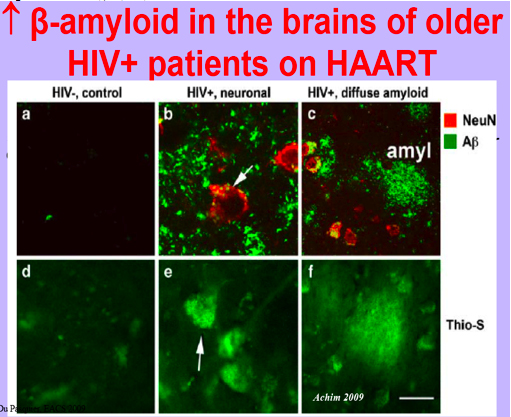
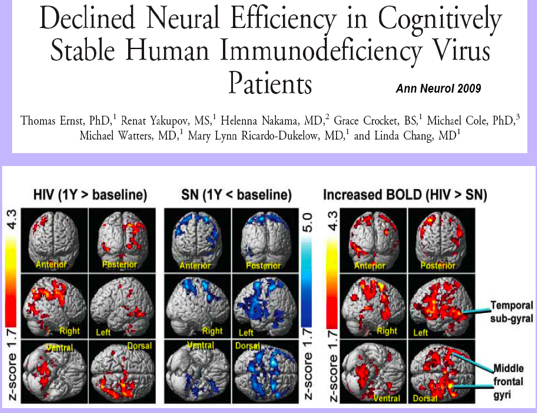
Fig. 3. Statistical parametric maps of changes in brain activation over the course of 1 year for human immunodeficiency virus (HIV)-positive (left) and seronegative (SN) controls (center) for the four-ball tracking task. Significant blood oxygen level dependent (BOLD) signal increases are indicated by Z-scores shown in the red-yellow scale and decreases by Z-scores on the blue-white scale. The HIV group shows only increases in brain activation, whereas the controls show only signal decreases after 1 year. The opposite changes led to significant interactions in brain activation between HIV status and time, with greater 1-year BOLD signal increases in HIV patients compared with SN controls (right). These findings suggest a practice effect in the controls but neural compensation in the HIV group to maintain performance. Clusters with greater than 300 voxels and p corrected 0.05 (voxel level) are shown.
All patients underwent a neuropsychological testing. We assessed general cognitive function using the HDS and the National Adult Reading Test which is an estimation of premorbid intelligence. Then, we tested more specifically attention, processing speed, working memory, and executive functions. We also added questionnaires measuring mood disorders, neuropsychiatric symptoms and QoL (MOS). Neuropsychological scores were compared to published norms adjusted for age, gender and education.
After the cognitive testing, patients were classified as having normal exam or ANI, MND or HIV-D if they fulfilled the criteria of the American Academy of Neurology AIDS Task Force.
Our AIMS were:
To determine the value of cognitive complaints in HIV+ patients
To determine the prevalence of HAND in HIV+ patients with long-lasting aviremia and with as few as confounding factors as possible
To assess the usefulness of the HIV dementia scale as a screening tool of HAND
HAND was diagnosed in 74% of the cohort.
Objective evidence of HAND was more frequent in complaining than in non-complaining patients (84% vs. 64%, respectively; p<0.001).
Complaining patients were more likely to experience HAND producing interference in daily functioning (MND or HIV-D; *p<0.001).
That our prevalence is high compared to other studies refers to the fact that we are among the first to take ANI into accounts.
A Receiver Operating Characteristic (ROC) curve was calculated by means of a non parametric approach and was used to define the best cut-off score for the HDS for the detection of any degree of HAND.
A threshold of 10 points classically defined for the detection of HIV-D,

from Jules: there may be irreparable damage from HIV early on after initial infection that not just persists but might get worse for certain individuals particularly those unable to normalize CD4, who have detectable viremia, with HCV coinfection and ciirhosis, those with additional risk factors including hypercholesterol/glycemia/smoking/fatty diet/genetics/drug use history.
|
| |
|
|
|
|
|