 |
|
|
| |
New fracture independently boosts death risk in big US HIV cohort
|
| |
| |
Conference on Retroviruses and Opportunistic Infections (CROI), March 4-7, 2019, Seattle
Mark Mascolini
WEBCAST: http://www.croiwebcasts.org/console/player/41069?mediaType=slideVideo&&crd_fl=0&ssmsrq=1554209341166&ctms=5000&csmsrq=5271
Prospective study of 6853 US adults with HIV independently linked a new (incident) fracture to a 45% higher risk of death from any cause [1]. Mortality after fracture dropped steeply across the 2000-2017 study period. Other mortality predictors in people with incident fracture were chronic kidney disease, HCV coinfection, non-AIDS cancer, and lung disease.
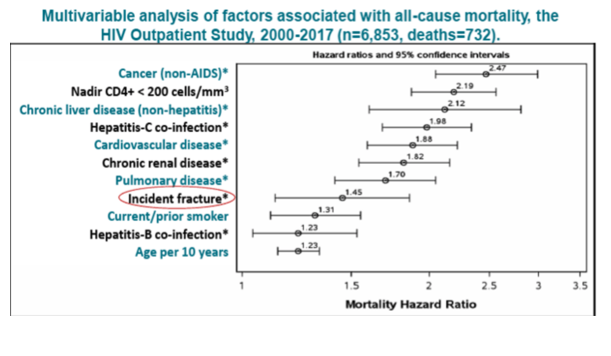
[also you can see in Table below among the entire HOPS cohort of 6,853 there were 732 deaths, multivariate analysis of factors associated with all-cause mortality included: cancer (non-AIDS) 2.47 HR, nadir CD4 <200 2.19 HR, chronic liver disease (non-hepatitis) 2.12 HR, HCV coinfection 1.98 HR, cardiovascular disease 1.88 HR, chronic renal disease 1.82 HR, pulmonary disease 1.70, incident fracture 1.45 HR, current/former smoker 1.31 HR HBV coinfection 1.23 HR and age 1.23 HR - who said comorbidites don’t kill us sooner & equate to shorter lifespan & survival?????. Jules]
Compared with the general population, people with HIV have higher rates of low bone mineral density (BMD) and run a greater risk of fracture. But HIV Outpatient Study (HOPS) researchers who conducted the new analysis pointed out that the impact of fractures on mortality in HIV populations remains unknown. They conducted this study to calculate all-cause mortality in HOPS across four periods (2000-2004, 2005-2008, 2009-2012, 2013-2017) in analyses adjusting for age and sex. They also aimed to explore associations between fracture and mortality while adjusting for sociodemographic, behavioral, and clinical factors.
HOPS is a longitudinal HIV cohort that began enrolling people in 1993 and currently has participants at six active sites across the United States. This analysis focused on cohort members from 8 active or recently active sites who had at least two study visits between January 2000 and September 2017. Among 6853 people seen during that period, 506 (7.4%) had a new fracture. Researchers used Cox proportional hazards models to (1) explore associations between incident fracture and mortality in all 6853 participants, and (2) identify mortality predictors in the 506 people who broke a bone.
People with a new fracture were older than those without a fracture when observation began (median 43 vs 39 years, P < 0.001), more likely to be a current or prior smoker (61% vs 53%, P = 0.001), more likely to drink more alcohol (P = 0.003), and more likely to have an AIDS diagnosis (55% vs 48%, P = 0.002). More time had passed since HIV diagnosis in the fracture group (median 5.5 vs 4.5 years, P = 0.019).
During follow-up, 732 of 6853 people (10.7%) died. Multivariable analysis indicated that breaking a bone during follow-up was independently associated with a 45% higher all-cause death risk (hazard ratio [HR] 1.45). Ten other factors also independently boosted the risk of death in the overall group, 7 of them at higher hazard ratios than incident fracture: non-AIDS cancer (HR 2.47), nadir CD4 count below 200 (HR 2.19), nonhepatitis chronic liver disease (HR 2.12), HCV coinfection (HR 1.98), cardiovascular disease (HR 1.88), chronic kidney disease (HR 1.82), pulmonary disease (HR 1.70), current/prior smoking (HR 1.31), HBV coinfection (HR 1.23), every 10 years of age (HR 1.23).
Among 506 people with incident fracture, 22 of the 75 who died (29.3%) had a major osteoporotic fracture and 53 (70.7%) had fractures at other sites. Mortality measured 1.65 per 100 person-years in those with osteoporotic fracture and 1.24 per 100 person-years in those with other fractures. The researchers defined osteoporotic fractures as those of the wrist, spine, hip/pelvis, or shoulder.
In an analysis adjusted for age and sex, mortality after a fracture dropped significantly across the four study periods: 8.46 per 100 person-years in 2000-2004, 2.97 per 100 in 2005-2008, 2.25 per 100 in 2009-2012, and 1.90 per 100 in 2013-2017 (P < 0.001).
Among the 506 people with a new fracture, four factors independently predicted death: chronic kidney disease (HR 2.85, 95% confidence interval [CI] 1.75 to 4.65, P < 0.001), HCV coinfection (HR 2.73, 95% CI 1.67 to 4.44, P < 0.001), non-AIDS cancer (HR 2.13, 95% CI 1.21 to 3.73, P = 0.009), and pulmonary disease (HR 2.07, 95% CI 1.27 to 3.38, P = 0.003). Every 10 years of age at the time of fracture also tended to boost the risk of death (HR 1.20, 95% CI 0.94 to 1.54, P = 0.15).
Reference
1. Battalora L, Armon C, Palella FJ, et al. Breaking bones is bad: incident fracture and mortality in the HIV Outpatient Study. Conference on Retroviruses and Opportunistic Infections (CROI). March 4-7, 2019. Seattle. Abstract 30.
CROI: BREAKING BONES IS BAD: INCIDENT FRACTURE AND MORTALITY IN THE HIV OUTPATIENT STUDY - 45% Increased Mortality Associated with Fracture - (03/06/19)
|
| |
|
|
|
|
|