 |
|
|
| |
Initial Weight, Low CD4/CD8, Low Activity Drive Weight Gains After InSTI Switch
|
| |
| |
CROI 2020, March 8-11, 2020, Boston
Mark Mascolini
A comparison of 281 adults who did or did not switch to an integrase inhibitor (InSTI) found that three factors explained weight gains substantially more than substituting an InSTI for another drug: higher initial weight, low CD4/CD8 ratio, and physical inactivity [1].
A continuing stream of studies records concerning rates of excess weight gains in HIV-positive people starting or switching to an InSTI. Because numerous other factors can contribute to weight gain or loss, researchers at Italy's Modena HIV Metabolic Clinic and collaborators in the United States conducted this study of 281 adults who did or did not substitute an InSTI for another drug in their regimen, without changing other antiretrovirals.
The primary aim was to figure the population-attributable fraction (PAF) [2] of modifiable factors in people who had a 5% or greater weight gain over an average 4 years of follow-up. This retrospective longitudinal study involved antiretroviral-treated people with an undetectable viral load while attending the HIV Metabolic Clinic between January 2007 and July 2019. When the observation period began, no one had taken an InSTI. During follow-up, people who substituted an InSTI for another antiretroviral were matched by age, sex, follow-up duration, and initial body mass index (BMI) to people who maintained their current regimen.
The researchers defined a significant weight gain as an increase of 5% or more from the first study visit through an average 4 years of follow-up. They recorded physical activity by the International Physical Activity Questionnaire as METs (metabolic equivalent of task). And they estimated daily caloric intake via 3-day food diary.
The 281 participants, 74% of them men, averaged 54.3 years in age and 4.2 years of follow-up. Median time taking antiretrovirals measured 22.3 years, and median CD4 count stood at 714. Almost everyone had an undetectable viral load.
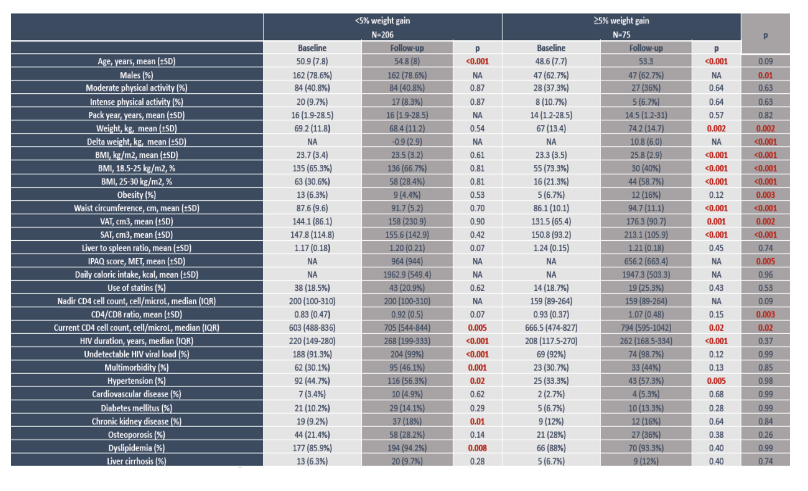
During follow-up, 118 people (42%) swapped one antiretroviral for an InSTI and 163 did not. The switchers has "a more pronounced immunological scar" marked by a lower nadir CD4 count (median 158 versus 220, P = 0.002), lower current CD4 count (median 578 versus 653, P = 0.009), lower CD4/CD8 ratio (0.79 versus 0.92, P = 0.04), longer HIV duration (median 244 versus 189 months, P < 0.001), and a higher proportion with multimorbidity (37% versus 25%, P = 0.04). The two groups did not differ significantly in age, physical activity, body mass index, waist circumference, or visceral or subcutaneous adipose tissue.
During follow-up, 75 people (27%) had a 5% or greater weight gain. From baseline to the last follow-up point, the weight gainers had significant changes in weight (67 to 74.2 kg, P = 0.002), BMI (23.3 to 25.8 kg/m2, P < 0.001), waist circumference, visceral and subcutaneous adipose tissue, CD4 count (666 to 794, P = 0.02), and proportion with hypertension (33% to 57%, P = 0.005).
Population-attributable fraction for weight gain proved greatest for initial BMI in overweight/obese range (45%, P < 0.001), CD4/CD8 ratio below 1 (41%, P < 0.001), and low physical activity (MET below 600, 32%, P < 0.02). These were the only statistically significant factors. Switching to an InSTI versus not switching contributed nonsignificantly to weight gain (P = 0.50), with a population-attributable fraction of 11%.
Both obesity and overweight at baseline boosted chances of more than a 5% weight gain during follow-up. The third most important weight-gain factor, low physical activity (MET below 600 at baseline), goes hand-in-hand with weight.
The researchers urged colleagues to recommend moderate to intense physical activity (MET above 600) to prevent weight gain. They suggested that such a program might include (1) 3 or more days of vigorous-intensity activity and/or walking for at least 30 minutes per day, or (2) 5 or more days of moderate-intensity activity and/or walking for at least 30 minutes per day, or (3) 5 or more days of any combination of walking, moderate-intensity, or vigorous-intensity activity.
References
1. Guaraldi G, Milic J, Malagoli A, et al. Contribution of InSTI, BMI, physical activity, caloric intake to weight gain in PWH. Conference on Retroviruses and Opportunistic Infections (CROI). March 8-11, 2020. Boston. Abstract 675.
2. The World Health Organization defines population-attributable fraction (PAF) as "the proportional reduction in population disease or mortality that would occur if exposure to a risk factor were reduced to an alternative ideal exposure scenario (eg. no tobacco use)." World Health Organization. Health statistics and information systems. Metrics: Population attributable fraction (PAF).
https://www.who.int/healthinfo/global_burden_disease/metrics_paf/en/
-------------------------------------------
poster pdf attached
Contribution of INSTI, BMI, physical activity or caloric intake to weight gain in PWH
Guaraldi G1, Milic J1, Malagoli A1, Carli F1, Menozzi M1, Franconi I1, Raimondi A1, Ciusa G1, Masi V1, Belli M1, Guaraldi S1, Mussini C1, Brown TT2, Lake JE3, Erlandson K4
1 Modena HIV Metabolic Clinic, University of Modena and Reggio Emilia, Modena, Italy; 2 Division of Endocrinology, Diabetes, and Metabolism, Department of Medicine, Johns
Hopkins University, Baltimore, Maryland; 3 University of Texas Health Sciences Centre, Houston, Texas, USA; 4 University of Colorado, Department of Medicine, Aurora, CO
|
| |
|
|
|
|
|