 |
|
|
| |
Is Liver Toxicity a CCR5 Antagonist Class Effect?
2NN & Hepatoxicity; D.A.D. study & liver related death; Liver toxicity & HIV, Italian study
|
| |
| |
A Report from the 10th European AIDS Conference (EACS), November 17-20, 2005, Dublin
Mark Mascolini
No one knows the answer to the question posed in this review's title. But an unscheduled addendum to an add-on talk in the EACS side effects session raised that grisly possibility.
The add-on talk came from Glaxo's Helen Steel, who explained in exacting detail why the company dismantled the development machine behind aplaviroc, Glaxo's CCR5 antagonist. The unscheduled addendum came from a Pfizer spokesman in the audience, prodded to the microphone by HIV and liver expert Stefan Mauss of Düsseldorf. Mauss asked for anyone from Pfizer to comment on swirling reports that serious liver toxicity had struck someone taking maraviroc.
A fellow from Pfizer read this prepared statement:
"Over a thousand patients have been enrolled in the maraviroc program to date. Pfizer has very recently become aware of a single case of hepatotoxicity in a patient receiving maraviroc. As the patient was also simultaneously receiving several drugs which have reported hepatic toxicities, the causality is unclear.
"Pfizer is still gathering more information regarding this patient and has called an additional review by the independent Data Safety Monitoring Board (DSMB) of the maraviroc program. While this review is awaited we are providing all patients, investigators, ethics committees and regulatory authorities with currently available information. We will comment further when we receive feedback from the DSMB and regulatory authorities."
The Pfizer spokesman declined to take questions.
Those who haven't been following the CCR5 antagonist saga should know the background for this unwelcome bomblet. Clinical trials of Pfizer's maraviroc, Glaxo's aplaviroc, and Schering's vicriviroc had been sailing along with few ill winds of late. Most concern focused on two questions:
- Would drugs that smother the CCR5 coreceptor on CD4 cells prod the protean virus to shift coreceptor allegiance and start hooking onto CXCR4, the coreceptor that arises in about half of people with late-stage HIV infection?
- Would virus resistant to one CCR5 antagonist prove cross-resistant to the others?
HIV's vexing capacity to do the right thing for itself and the wrong thing for patients suggests the answers could be yes, though evidence of "coreceptor switching" has been sparse in the limited clinical trials to date.
Then Glaxo put a chill on warm hopes for aplaviroc when severe hepatotoxicity arose in a few antiretroviral-naive people taking the drug. The company promptly shut down that trial and looked hard for sick liver signals in treatment-experienced people taking aplaviroc. Glaxo found exactly what everyone hoped it wouldn't—the same kind of liver toxicity in experienced people taking aplaviroc with other antiretrovirals for salvage.
What sunk aplaviroc
Why would a bare handful of liver problems—four, as it turned out—bring a megabucks clinical trial juggernaut to a clanging halt? Because, Glaxo's Steel explained, liver experts figure that the specific type of toxicity they saw will kill 10% to 50% of those who have it.
No one in the Glaxo trials died, and the toxicity always resolved when they stopped aplaviroc. When researchers rechallenged one of these people with aplaviroc and Combivir (AZT/3TC), signals of hepatic distress arose again.
All four people had elevated alanine aminotransferase (ALT)—sometimes sky-high ALT—plus simultaneously soaring bilirubins. The FDA lists an ALT more than 3 times the upper limit of normal (ULN) plus total bilirubin more than 1.5 times ULN as a "cause for concern."
The trial enrollee who alerted Glaxo to the liver threat had an ALT 70 times ULN and a bilirubin 5 times ULN after taking aplaviroc and Combivir for 59 days. He did not have HBV or HCV coinfection and started the trial with a normal ALT, aspartate aminotransferase (AST), and bilirubin. Nothing else in his medical history suggested why his ALT might suddenly spike to nosebleed heights. Liver biopsy showed a chronic inflammatory infiltrate "consistent with drug-induced hepatotoxicity."
Scouring the central lab database on aplaviroc for similar cases, Glaxo found three it could attribute to the CCR5 antagonist, including one with an ALT 24 times ULN, one with an ALT 12 times ULN, and one with an ALT and AST 9 times ULN.
Although only four of 308 aplaviroc trial enrollees met the criterion of simultaneous high ALT and bilirubin, that was four too many. Glaxo had no choice but to pull the plug on aplaviroc.
What's up with maraviroc?
Pfizer says it wants to alert trial participants and investigators to the single liver toxicity case it found before disseminating the findings publicly. NATAP will report full details as soon as they become available.
That even one such case arose came as a rude surprise since DSMBs for maraviroc trials had just finished a hair-splitting scrutiny of ongoing trials and found nothing that encouraged them even to tinker with the trial protocols.
Liver readings did jog out of line in 5 of 12 healthy volunteers taking maraviroc for 8 days with tipranavir/ritonavir in a pharmacokinetic study [1]. Pfizer planned this study to address the concern that inhibitors or inducers cytochrome P450 (CYP) enzymes—the enzymes responsible for metabolizing so many drugs—affect maraviroc concentrations.
Pfizer has already decided to halve maraviroc's dose when giving it with puissant inhibitors of CYP3A4 like ritonavir. But tipranavir is a CYP3A4 inducer. So Pfizer wanted to know how standard-dose tipranavir/ritonavir (500/200 mg twice daily) might affect 150 mg of maraviroc (the half dose) twice daily.
Pfizer's Samantha Abel and colleagues gave the volunteers that dose of maraviroc with either placebo or tipranavir/ritonavir for 8 days. Later the volunteers switched to the regimen they hadn't already tried.
Tipranavir/ritonavir did not change maraviroc levels enough to merit a dose adjustment. But these healthy volunteers had more side effects when taking maraviroc with the protease inhibitors (PIs) than when taking it with placebo.
Most notably, 5 of 12 people taking maraviroc with the PIs had elevated ALT or AST after 8 days of dosing. Four of these transaminase jumps rated as grade 1 or 2 elevations, and one ranked as a more serious grade 3 change. No one in the trial had simultaneous surges in bilirubin—the cofactor that killed aplaviroc.
All transaminase elevations vanished spontaneously when people stopped maraviroc and the PIs. Tipranavir/ritonavir can certainly pummel the liver in people with HIV, and liver toxicity did not arise with maraviroc plus placebo. So this study cannot pin the liver enzyme blips on maraviroc.
Still, no one can be happy about the unpropitious proportion of ALT or AST leaps in these healthy people, 42% Grade 1 or 2 "events" may not seem troubling, but these healthy people took maraviroc and tipranavir/ritonavir for only 8 days. In the red-alert case from the aplaviroc trial, liver enzymes looked just fine for 58 days.
Even if maraviroc didn't stir up liver enzymes all by itself—as aplaviroc did—a drug that compounds liver toxicity from other antiretrovirals would have a more limited salvage role or—at a minimum—would require tight monitoring.
So far Schering has reported no liver toxicity with its CCR5 antagonist, vicriviroc. But the company shuttered a trial in previously untreated people when vicriviroc plus Combivir trailed efavirenz plus Combivir in slowing HIV replication [2].
At an October IAPAC meeting in Amsterdam, Joep Lange from the Academic Medical Center noted that AZT spurred emergence of CXCR4-favoring HIV in monotherapy trials. Whether drugs with that trait are the best partners for CCR5 antagonists remains unexplored. Schering plans to keep testing vicriviroc in treatment-naive people with a partner other than Combivir.
Will hepatotoxicity prove to be a CCR5 antagonist class effect? The optimist would say toxic class effects are the exception rather than the rule. Nucleosides differ considerably in how mess up mitochondria; efavirenz does not induce the acute liver toxicity seen with nevirapine; and PIs differ in how they affect lipid levels and glucose control. The pessimist would say don't rule anything out until you have lots of data from lots of people.
Liver toxicity of unknown origin associated with HIV-infection
Assaults on the liver are bad enough when you know their cause. But research from Spain and Italy suggests severe liver disease with no known origin besets about 1 in 200 people with HIV [3]. Some EACS attendees questioned the study's methods.
Ivana Maida (University of Sassari, Italy) and colleagues in Madrid and Seville combed records of 3200 people with HIV infection, defining liver disease of unknown origin as persistently high ALT or AST without replicative HBV or HCV infection or another known cause of liver problems. Seventeen people (0.5%) met that definition, while the rate in the general population lies below 0.01%. To flush out possible contributors to the condition, Maida matched these 17 people to HIV-infected controls on the basis of age, gender, and CD4 count.
Fourteen people with unexplained transaminase spurts (82%) were men, and 13 men picked up HIV from sex with other men. The 17 people with a high ALT or AST had a median age of 42 years and had HIV infection for a median of 15 years. The most common potentially hepatotoxic drugs on their charts were nevirapine, ddI, and d4T.
Nine of the 17 people had portal hypertension, 6 had portal thrombosis, 5 had gastrointestinal bleeding, and 2 had hepatic encephalopathy. No one died. Liver biopsy or the noninvasive Fibroscan rated fibrosis advanced (Metavir score F3 or F4) in 7 cohort members.
People with liver toxicity differed from the controls without it in having less antiretroviral experience (4.53 versus 6.88 years, P = 0.02) but more ddI experience (47 versus 25 months, P = 0.009). Cases and controls did not differ in length of treatment with d4T or nevirapine, or in any other variable measured.
Multivariate analysis singled out a solitary factor that independently raised the risk of unexplained liver problems: Taking ddI upped the odds 1.04 times for every month of treatment.
Maida noted that the analysis cannot rule out other explanations of liver upsets in this population. Most of those affected, she explained, were gay men, and gay men have higher rates of pylephlebitis (inflammation or thrombosis of the liver's portal vein) than do other people with HIV.
Stefan Mauss raised the concern that excluding people with nonalcoholic steatohepatitis and hepatic steatosis from the analysis may have made it impossible to spot correlations between antiretroviral therapy and a compromised liver. Another attendee questioned the fibrosis finding, arguing that research has not validated Fibroscan in people with HIV and the test may be accurate only in those with advanced fibrosis.
High 2NN liver toxicity rates with
once-daily nevirapine tied to Thai site
After-the-fact analysis of data from the 2NN trial [4] showed that the high rates of liver toxicity seen with once-daily nevirapine could be traced largely to the single Thai site in this international study [5]. At other sites rates of symptomatic and asymptomatic liver toxicity did not vary significantly when researchers compared people taking once-daily nevirapine, twice-daily nevirapine, or efavirenz—after accounting for pretreatment CD4 count—in this randomized trial of people starting antiretroviral therapy.
Boehringer Ingelheim's Jonathan Leith and colleagues defined asymptomatic liver toxicity as an ALT or AST at least 5 times ULN without symptoms of clinical hepatitis.
In the overall 2NN population, rates of symptomatic and asymptomatic liver toxicity were highest with once-daily nevirapine, lower with twice-daily nevirapine, and lowest with efavirenz (Table). The analysis excluded 2NN's nevirapine-plus-efavirenz arm.
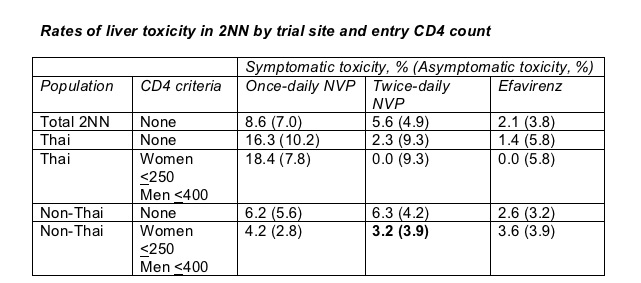
When Leith divided results between Thai and non-Thai trial sites, rates of symptomatic and asymptomatic liver toxicity were higher with once- or twice-daily nevirapine than with efavirenz in both Thai and non-Thai groups (Table). But when Leith looked only at non-Thai trial participants who began nevirapine at currently recommended CD4 counts (below 250 cells/mL for women and below 400 cells/mL for men), toxicity differences between the three arms disappeared.
The Boehringer researchers did not speculate on whether the higher nevirapine toxicity seen in the single Thai center might be explained by some genetic difference between Thais and other study participants or whether the Thai site differed from others in recording or reporting hepatotoxicity. Leith and colleagues point out that other trials with a once-daily nevirapine arm charted lower ALTs and ASTs than those recorded in 2NN and did not see the high rates of asymptomatic liver toxicity reported from Thailand [6-9]. The FDA has not licensed nevirapine for once-daily use.
Antiretrovirals not a factor in D:A:D liver deaths
Longer experience with antiretroviral therapy did not raise the risk of liver-related death in the multicohort D:A:D study, but lower CD4 counts did make death from liver disease more likely [10]. Rainer Weber (University Hospital, Zurich) and D:A:D coworkers caution, though, that antiretrovirals' salutary (beneficial) effect on CD4 tallies could mask a detrimental antiretroviral impact on the liver.
Tracing causes of death in 1248 D:A:D participants (5.3%), Weber found that AIDS explained the largest proportion of deaths (31%) from 2000 through February 2004, followed by liver failure (15%), heart disease (9%) and non-AIDS malignancies (9%).
Among people who died from liver disease, Weber traced 76% of the deaths to viral hepatitis (66% HCV and 17% HBV), 9% to hepatocellular carcinoma, and 14% to alcohol abuse.
Univariate analysis of liver death risk factors did not link cumulative antiretroviral duration—up to 7 years' worth—to liver-related death. Multivariate analysis tied five variables to a higher risk of liver-related death at the following relative rates (and 95% confidence intervals):
- Older age: 1.3 (1.2 to 1.4) per 5 years older
- HIV transmission group: 2.0 (1.2 to 3.4) for injecting drug use versus homosexual infection
- Lower CD4 count: 1.23 (1.17 to 1.29) per halving of the latest CD4 count (P < 0.0001)
- HCV infection: 6.7 (3.9 to 11.2)
- HBV antigen positive: 3.7 (2.4 to 5.9)
In an attempt to uncover any negative antiretroviral impact on liver mortality, in future analyses D:A:D number crunchers will weigh years of antiretroviral therapy and risk of liver-related death after adjusting for the latest CD4 count.
Mark Mascolini writes about HIV infection (markmascolini@earthlink.net).
References
1. Abel S, Taylor-Worth R, Ridgway C, et al. Effect of boosted tipranavir on the pharmacokinetics of maraviroc (UK 427,857) in healthy volunteers. 10th European AIDS Conference. November 17-20, 2005. Dublin. Abstract LBPE4.3/15.
2. Schering-Plough. Schering-Plough discontinues phase II study of vicriviroc in treatment-naive HIV patients, continues phase II study in treatment-experienced HIV patients. October 27, 2005. http://www.aegis.org/news/pr/2005/PR051044.html
3. Maida I, Nuñez M, Rios MJ, et al. Severe liver disease of unknown origin in HIV-infected patients. 10th European AIDS Conference. November 17-20, 2005. Dublin. Abstract PS5/5.
4. van Leth F, Phanuphak P, Ruxrungtham K, et al. Comparison of first-line antiretroviral therapy with regimens including nevirapine, efavirenz, or both drugs, plus stavudine and lamivudine: a randomised open-label trial, the 2NN Study. Lancet 2004;363:1253-1263.
5. Storfer S, Leith J, Piliero P, Hall D. Analysis of hepatic events within the 2NN study: controlling for ethnicity and CD4+ count at initiation of nevirapine therapy. 10th European AIDS Conference. November 17-20, 2005. Dublin. Abstract PE9.6/2.
6. van Leeuwen R, Katlama C, Murphy RL, et al. A randomized trial to study first-line combination therapy with or without a protease inhibitor in HIV-1-infected patients. AIDS 2003;17:987-999.
7. Garcia F, Knobel H, Sambeat MA, et al. Comparison of twice-daily stavudine plus once- or twice-daily didanosine and nevirapine in early stages of HIV infection: the scan study. AIDS 2000;14:2485-2494.
8. Raffi F, Reliquet V, Ferre V, et al. The VIRGO study: nevirapine, didanosine and stavudine combination therapy in antiretroviral-naive HIV-1-infected adults. Antivir Ther 2000;5:267-272.
9. Negredo E, Molto J, Munoz-Moreno JA, et al. Safety and efficacy of once-daily didanosine, tenofovir and nevirapine as a simplification antiretroviral approach. Antivir Ther 2004;9:335-342.
10. Weber R, Friis-Moller N, Sabin C, et al. Liver-related deaths among HIV-infected persons: data from the D:A:D study. 10th European AIDS Conference. November 17-20, 2005. Dublin. Abstract PE18.4/7.
|
|
| |
| |
|
|
|
|
|