| |
Lack of Evidence of Sexual Transmission of Hepatitis C Virus in a Prospective Cohort Study of Men Who Have Sex With Men
|
| |
| |
March 2005, American Journal of Public Health
Michel Alary, MD, PhD, Jean R. Joly, MD, FRCPC, MSPH, MBA, Jean Vincelette, MD, MSc, FRCPC, Rene Lavoie, BA, Bruno Turmel, MD and Robert S. Remis, MD, MPH, FRCPC
Michel Alary is with the Unite de recherche en sante des populations, Centre hospitalier affilie universitaire de Quebec and Universite Laval, Quebec City, Quebec. Michel Alary and Bruno Turmel are with the Institut national de sante publique du Quebec, Quebec and Mon-treal, Quebec. Jean R. Joly is with the Laboratoire de sante publique du Quebec, Sainte-Anne-de-Bellevue, Quebec. Jean Vincelette is with the Service de microbiologie, Centre hospitalier de l'Universite de Montreal, Hopital St-Luc, Montreal, Quebec. Rene Lavoie is with Action Sero-Zero, Montreal. Robert S. Remis is with the Department of Public Health Sciences, University of Toronto, Toronto, Ontario.
Note from Jules Levin: In AIDS journal Nov 2005 researchers report finding HCV in the semen of men coinfected with HCV & HIV more frequently than in the semen of HCV monoinfected men (37% vs 18%; p=0.033). The coinfected men with HCV+ semen had significantly higher HCV blood load than men with HCV- semen, which could explain why the coinfected men had a higher prevalence of HCV in semen than non-coinfected men. This report fuels the controversy of whether HCV can be transmitted sexually, among MSM and among heterosexuals. Many anecdotal reports in the USA support the notion that HCV can be transmitted sexually among heterosexual couples when one partner has HIV. Studies find that sexual HCV transmission is facilitated by the presence of STDs. Traumatic sex may increase risk for transmission. Reports from conferences and publications find increased cases of acute HCV among MSM in the UK & France. The researchers report with confidence that injection drug use is not the cause. It is therefore suggested that the presence of STDs & higher HCV viral loads among HIV+ individuals may be the reasons for HCV sexual transmission. Of interest is the study reported in this article, but bear in mind this study was conducted 4 years ago. Lifestyle practices may be different in Montreal in 2001 than in the UK & Paris in 2005.
ABSTRACT
Objectives. We studied the prevalence and incidence of hepatitis C virus (HCV) infection in the ongoing Omega Cohort Study of men who have sex with men (MSM).
Methods. From January to September 2001, consenting men (n = 1085) attending a follow-up visit to the ongoing Omega Cohort Study were tested for HCV. If the test results were positive for HCV, we compared them with test results from previous serum samples collected from the time of entry into the original cohort study to determine the time of infection.
Results. HCV prevalence at entry was 2.9% and was strongly associated with injection drug use (32.9% vs 0.3%, P<.0001). Only 1 seroconversion was identified in 2653 person-years of follow-up (incidence rate = 0.038 per 100 person-years). The seroconverter was an active injection drug user who reported needle sharing.
Conclusions. Sexual transmission of HCV among MSM appears to be rare.
INTRODUCTION
The occurrence of sexual transmission of the hepatitis C virus (HCV) is still highly debated.1-3 Case reports of sexual transmission of HCV have been documented,4-6 but epidemiological studies of the associations between different sexual behaviors and HCV transmission have produced divergent results.1,7
These discrepancies may be explained by the low risk of transmission, the use of prevalence and case report studies to ascertain transmission, and the lack of appropriate control groups. In some cases, potentially important exposures might not have been included in the study questionnaires (e.g., the use of glass syringes for injections of medications, tonics, or both in Italian couples before the 1970s1). Additional limits to the validity of earlier reports are first-generation serological tests and the small size of many studies. Hence, if sexual transmission of HCV is indeed inefficient, many of these studies may well have lacked an adequate sample size to demonstrate transmission or to evaluate the risk of transmission. Given these caveats, it is not surprising that the results are conflicting. Biologically, transmission is possible, because viral RNA has been found in saliva, semen, and vaginal secretions.8,9
Sexual transmission of HCV among men who have sex with men (MSM) has not been studied as extensively as has sexual transmission in heterosexual couples. In prevalence studies conducted in a STD clinic in London, Tedder et al.10 observed a greater prevalence of HCV antibodies among MSM than among heterosexuals (2.2%, 95% confidence interval [CI] = 0.5, 4.0 vs 0.8%, CI = 0.0, 1.8). When injection drug users (IDUs) were excluded, this difference was no longer present.7,10 Other studies of MSM have found HCV antibody prevalences of 4.6% (United States11), 6.9% (Italy,12), and 1.4% (Denmark13).
Balasekaran et al.,14 Delage et al.,15 and Buchbinder et al.16 found no association between sexual orientation (heterosexual vs homosexual) and the presence of HCV antibodies. Similarly, Osella et al. were unable to find an association between any sexual behavior and the transmission of HCV among 228 MSM.17 Finally, 2 cross-sectional studies suggested an association between specific MSM sexual practices and HCV infection, but these associations either disappeared in the multivariate analysis18 or were only borderline significant.11
The issue of sexual transmission of HCV infection was reviewed by Terrault in 2002.19 We examined the transmission of HCV in a large cohort of MSM in Montreal as an offshoot of the Omega Cohort Study.
Participants
The Omega Cohort Study is an ongoing, open prospective cohort in which risk factors associated with the transmission of HIV among MSM in Montreal are being evaluated (recruitment began in October 1996). Study objectives also include characterizing changes in sexual behavior over time and identifying psychosocial factors associated with risky sexual behavior. Serum samples are collected every 6 months, and an extensive questionnaire on all known risk factors associated with HIV transmission is completed at the time of the serum sample collection.
From January 4 to September 8, 2001, all men presenting for a follow-up visit were asked to participate in the HCV transmission study (n = 1085). After consent was obtained, a blood sample was collected and tested for HCV. If the result was negative, no further testing for HCV was performed. If the result was positive, the serum specimen obtained at entry into the Omega Cohort Study (T0) was tested for the presence of HCV antibodies. If the result obtained on this sample was also positive, the participant was not included in the incidence study. If the result was negative at T0, all available serum samples were tested to determine the probable time of infection.
The Omega Cohort Study questionnaire is extensive with respect to the probable transmission routes for HCV, and it is exhaustive with respect to sexual practices. Questions about previous blood transfusion, drug usage (e.g., parenteral, snorted), and other less likely routes of transmission (e.g., tattoo, body piercing) are included in the semiannual interviews.
Laboratory Procedures
Initial screening of serum samples was performed with the COBAS CORE Anti-HCV Enzyme Immunoassay II (third-generation assay; Roche Diagnostics, Branchburg, NJ). Reactive samples were then retested with an enzyme immunoassay (Axsym HCV version 3.0, Abbott Laboratories, Mississauga, Ontario) with a more stringent criterion (sample/ cut-off [index] 10 vs 1). These criteria are more stringent than those currently accepted by the US Centers for Disease Control and Prevention. All samples reactive to the screening test were confirmed in this way, with the exception of 4 samples that had an index of less than 10. These 4 samples were confirmed to be positive at the Laboratoire de sante publique du Quebec with additional tests: a double enzyme immunoassay (Monolisa anti-HCV Plus, Sanofi Diagnostics Pasteur, Marne La Coquette, France, and Ortho HCV 3.0 enzyme-linked immunosorbent assay test with enhanced SAVe, Ortho Diagnostica, Raritan, NJ). Finally, the serum at enrollment and the first anti-HCV-positive serum of serocon-verters were tested for HCV RNA with COBAS AMPLICOR HCV test 2.0 (Roche Diagnostics, Branchburg, NJ). Positive samples according to the criteria mentioned above were considered to come from an infected (past or present) person. All tests included appropriate quality controls.
Statistical Analysis
The prevalence of HCV infection at entry into the cohort was computed and compared by risk factors with the Fisher exact test. Exact 95% confidence intervals of the prevalence figures, based on the binomial distribution, also were computed. For participants who were HCV-negative at baseline (T0), we calculated person-years of follow-up (1) from baseline to the first HCV-positive test for sero-converters and (2) until the visit occurring between January 4 and September 8, 2001, for those who remained HCV-negative. The allocation of person-years to different categories of risk factors accounted for the time-dependent nature of behavioral variables, with person-time for a given individual potentially attributable to different categories according to the modification in behavior reported between each follow-up questionnaire. We used an exact method based on the Poisson distribution to compute the 95% confidence intervals for the HCV incidence rates.
RESULTS
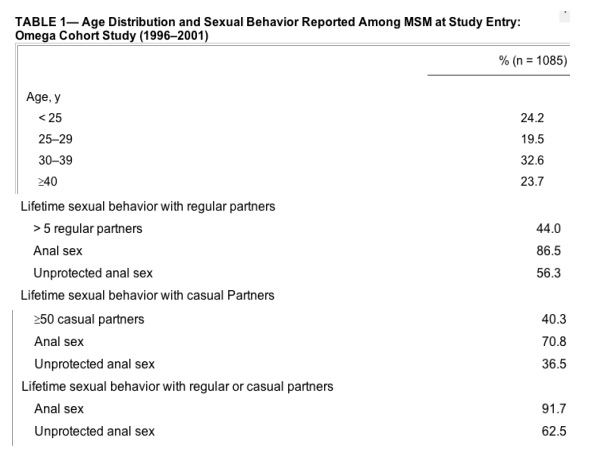
Median age was 32 years. A high proportion of participants reported large numbers of sexual partners during their lifetimes as well as unprotected anal intercourse.
Of the 1085 men who participated in the study, 32 were HCV-positive (2.9%; 95% CI = 2.0, 4.1). Thirty-one of these were found to have already been infected at T0, whereas 1 participant was identified as a seroconverter between his first and second follow-up visits. HCV RNA was detected in the seroconversion sample but not at T0.
Of the 85 participants with a history of injection drug use, 28 (32.9%) were HCV-positive at entry, compared with 3 (0.3%) HCV-positive among the 980 participants without such a history (P < .0001, Fisher exact test). HCV prevalence was also much higher among current IDUs than among former IDUs (47.6% vs 19.5%; P = .006, Fisher exact test). HCV prevalence was significantly higher among IDUs who reported previous needle sharing than among those who had never shared needles (48.0% vs 12.9%; P = .002, Fisher exact test). After control for injection drug use, lifetime and recent (past 6 months) sexual behavior (e.g., number of regular or casual partners, unprotected anal sex with both types of partners) were not significantly associated with prevalent HCV infection (all P > .1).
The 3 non-IDUs with HCV infection reported sexual behavior similar to that reported by HCV-negative participants. Moreover, 2 of the 3 reported 100% protected lifetime anal sex. One of the 3 reported a previous blood transfusion (date unknown) as well as body piercing; the other 2 reported risk factors that have been inconsistently associated with HCV in cross-sectional studies20: one reported frequent cocaine snorting, and the other reported occasional cocaine snorting and a history of body piercing. In addition, HCV prevalence was higher among non-IDUs with any of these 3 risk factors (cocaine snorting, blood transfusion, or body piercing), although not significantly so, because of small sample numbers (P values between .17 and .23, Fisher exact test). The actual prevalence figures (presence vs absence of factor) were as follows: cocaine snorting (0.78% vs 0.14%), blood transfusion (1.28% vs 0.24%), and body piercing (0.69% vs 0.15%).
The 1054 men who were HCV-negative at baseline contributed a total of 2653 person-years of follow-up. With only 1 seroconversion, the overall incidence of HCV infection was 0.038 per 100 person-years (95% CI = 0.001, 0.21). This seroconversion occurred in an IDU who reported needle sharing during the 6 months preceding the visit at which he first tested positive for HCV. The HCV infection incidence rate was 1 per 43 person-years among IDUs (95% CI = 0.06, 12.9) compared with 0 per 2610 person-years of follow-up among non-IDUs (95% CI = 0, 0.14).
DISCUSSION
The prevalence of HCV among MSM entering the Omega Cohort Study was 2.9%. This figure is somewhat lower than figures observed among MSM in the United States11 and in Italy12 but somewhat higher than prevalences found in studies in the United Kingdom10 and in Denmark.13 The HCV prevalence we observed among MSM in Montreal was only slightly higher than that among the general population of men in this city (2.3%, J. R. Joly, unpublished data, 1999). When we excluded IDUs from our study, the prevalence was only 0.3%, a figure lower than the overall estimation of 0.8% for HCV prevalence among the Canadian population.21 Discrepancies in prevalence estimates from previous studies in MSM may well depend on the proportion of participants who are IDUs. However, because the main objective of the Omega Cohort Study is to examine factors related to HIV seroconversion, the study selects for HIV-negative participants, who may be at lower risk for HCV infection than HIV-positive participants. Our findings therefore may underestimate the true HCV prevalence among Montreal MSM, including MSM IDUs.
Despite this possible underestimation, the level of sexual risk among the participants in the Omega Cohort Study was far from low. In addition, the prevalence of hepatitis B markers was 41% in unvaccinated participants at enrollment,22 a figure almost 15-fold greater than HCV prevalence. The prevalence of hepatitis B surface antigen was 4.3%. The incidence of HIV in the Omega Cohort Study was 0.56 per 100 person-years, a figure that is also approximately 15-fold greater than HCV incidence in the same cohort.23 HCV incidence among IDUs participating in the Omega Cohort Study was lower than that in previously reported studies.24,25 This low incidence may be a result of the small number of person-years of follow-up among IDUs in our study, which resulted in wide confidence intervals, or because of the possibility that a study recruiting MSM may select less-compulsive IDUs than are selected by studies in which the entry criterion is current injection drug use. Preventive counseling during follow-up also may have reduced HCV incidence among IDUs.
In a cohort study of 259 MSM followed in Denmark between 1981 and 1989,26 3 cases of HCV seroconversion occurred; only 1 of them occurred in an IDU. The 8-year cumulative incidence in this study was 4.1%. The discrepancy between these results and ours may be explained by the fact that, at the time of the Denmark study, only first-generation HCV antibody tests were available, and these older tests tended to have suboptimal specificity. Another possible explanation is that nonsexual risk factors other than injection drug use were not assessed in this study. Indeed, in our study, the 3 non-IDUs with prevalent cases reported such factors. The fact that several reviews on sexual transmission of HCV concluded that this virus can definitively be transmitted sexually,1,17,19 although with a low probability, could be attributable to underascertainment of potential nonsexual risk factors. However, the upper bound of the 95% confidence interval for HCV incidence among non-IDUs in our study (0.14 per 100 person-years) does not entirely exclude the possibility of low-level sexual transmission in MSM.
Thomas et al. reported a significant association between MSM and HCV (odds ratio [OR] = 3.61). When the analysis was restricted to MSM who reported engaging in anal receptive sex, the odds ratio was reduced to 2.3.18 However, all male participants, MSM and non-MSM, were included in these analyses. After incorporation of data from Thomas et al. and restriction of the analysis to the subset of MSM (38 participants), anal receptive sex appeared to have a protective effect (OR = 0.55). Furthermore, in the logistic regression model developed by these authors, the association of male homosexual exposure with anti-HCV became nonsignificant when HIV infection was included in the model, because 24 of 38 males (63.2%) with homosexual exposure were also HIV-positive. When HIV status was excluded from the model, homosexual exposure remained significantly associated with anti-HCV (P = .012). Thus, either the small number of MSM or the effect of HIV co-infection could explain the results of that study.
In a study by Osmond et al., the odds ratio linking a high number of lifetime sexual partners and HCV infection was 2.1 (95% CI = 0.9, 4.8), thus providing some evidence of sexual transmission of HCV among MSM.11
Despite the fact that ours was the largest cohort study on this topic, the power of our study to assess sexual transmission of HCV among MSM is low. This low power results from the low incidence we observed, suggesting that sexual transmission appears to be a rare event in this population. Further studies are needed to better delineate the role of other nonsexual and non-injection drug use risk factors in HCV transmission.
|
|
| |
| |
|
|
|