 |
|
|
| |
PI & NNRTI Drug Levels in Coinfected Patients
|
| |
| |
Reported by Jules Levin
"The HEPADOSE Study: Evaluation of protease inhibitors and non nucleoside analogue plasma concentrations in HIV/HCV and HIV-infected patients"
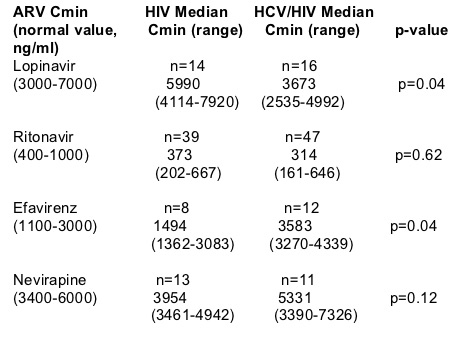
The study authors found that In HCV/HIV coinfected patients in this study Cmin "did not change significantly' for lopinavir, but the authors said NNRTIs "were strongly overdosed" in coinfected patients suggesting the need for drug monitoring in this population. Median Cmin for EFV was found here as 1494 ng/ml in HIV+ vs 3583 ng/ml in coinfected (p=0.04). Median NVP Cmin was found in this study to be 3954 ng/ml in HIV+ vs 5331 ng/ml in coinfected (p=0.12). The study found HIV-infected patients taking lopinavir had median Cmin levels of 5990 ng/ml vs 3673 ng/ml in HCV/HIV coinfected, p=0.04). These data were taken from the IAS Program Abstract Book. Further study is warranted for all HIV drugs to evaluate the effect in patients with HCV & HBV.
Dominguez S1, Peytavin G2, Guiget M1, Calvez V1, Costagiola D1, Bricaire F1, Poynard T1, Katlama C1, Benhamou Y1
1Pitie Salpetriere Hospital, INSERM unity U720, University Pierre and Marie Curie, Paris, France, 2Bichat Claude Bernard Hospital, Paris, France
French researchers reported at IAS-Rio results from this study of whether HCV/HIV coinfection could impair drug metabolism. Previous studies suggest liver impairment & heptatitis might slow HIV drug metabolism. But I think most of these studies are not conducted properly because they do not compare cirrhotic patients with those with little or no fibrosis so I'm not sure the results are applicable to all coinfected patients. This study did report differences in concentrations of NNRTIs between F4 stage and F0-F3 stage. The study authors suggest that this population of coinfected patients would benefit from TDM, which I agree with.
Methods: To compare plasma ARV concentrations in a cross-sectional study they performed plasma ARV concentrations (Cmin) in HCv/HIV coinfected patients with a documented liver biopsy within two years matched on HIV patients according to sex and ARV. They used the standard threshold value to define the NNRTI and PI expected therapeutic concentrations. Statistical analysis was performed by using non parametric Wilcoxon test, or Fishers's exact test.
The study authors reported these results:
They enrolled 73 HCV/HIV coinfected & 66 HIV infected patients, HIV RNA was <200 c/ml in 68% and 83% of patients, median CD4 count was 331 and 385, respectively. Median PI Cmin were similar in the two groups, except for lopinavir which was lower in coinfected patients. Both EFV & NVP Cmin were higher in coinfected compared to HIV-infected patients. Morover, according to the fibrosis stage NNRTI Cmin were significantly over the expected therapeutic concentration in HCV/HIV patients: 86% in F4 stage, 56% in F0-F3 stage compared to 24% in HIV patients (p=0.01). Among patients with NNRTI Cmin over the expected therapeutic concentration cytolysis grade 2 was significantly more frequent in HCV/HIV patients compared to HIV-infected patients (39% vs 10%) (p=0.02).
|
| |
|
|
|
|
|