 |
|
|
| |
ARTs to Prevent HIV Sexual Transmission
|
| |
| |
Reported by Jules Levin
First Dose and Steady-state Genital Tract Pharmacokinetics of Ten Antiretroviral Drugs in HIV-infected Women: Implications for Pre- and Post- Exposure Prophylaxis
Julie Dumond*, R Yeh, K Patterson, A Corbett, B H Jung, N Rezk, A Bridges, E Dempsey, M Cohen, and A Kashuba
Univ of North Carolina at Chapel Hill, US
Background: Antiretroviral (ARV) therapy has been shown to reduce GT HIV RNA and potentially decrease the risk of sexual transmission. ARVs rapidly achieving high GT concentrations (CONC) may be targets for optimal PREP and PEP. To assist in choosing the most appropriate regimens, this investigation comprehensively evaluated first dose and SS PK of 10 ARVs in the female GT (FGT).
Methods: A non-blinded, PK study was performed in 23 HIV-infected women initiating provider-selected ARVs including combinations of the following: lamivudine (3TC), zidovudine (ZDV), abacavir (ABC), emtricitibine (FTC), didanosine (ddI), stavudine (d4T), efavirenz (EFV), lopinavir (LPV), ritonavir (RTV), and atazanavir (ATV).
Six paired blood plasma (BP) and directly aspirated GT samples were obtained over a dosing interval around observed doses on Day 1 (D1) and after Day 21 (SS). BP and GT CONC were measured by validated LC/UV and LC/MS/MS assays.
Data were analyzed by noncompartmental PK and nonparametric statistical methods. GT:BP AUC ratios were calculated and are presented as median (IQR).
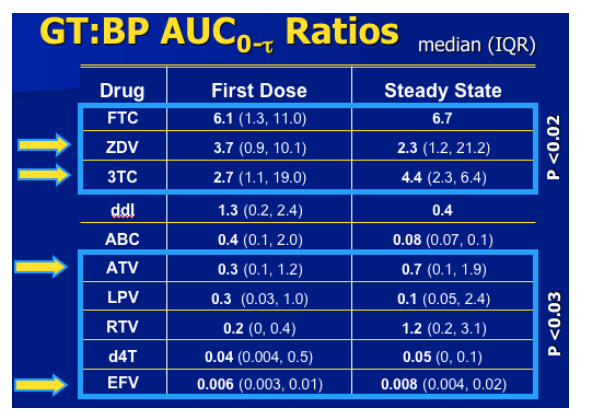
At D1 and SS, ZDV, 3TC, and FTC FGT exposures were higher than BP (p<0.02); d4T, RTV, EFV, LPV, and ATV GT exposures were less than BP (p<0.03). A trend towards higher FGT exposures on D1 compared to SS was noted for ZDV, ABC, and ddI (p=NS).
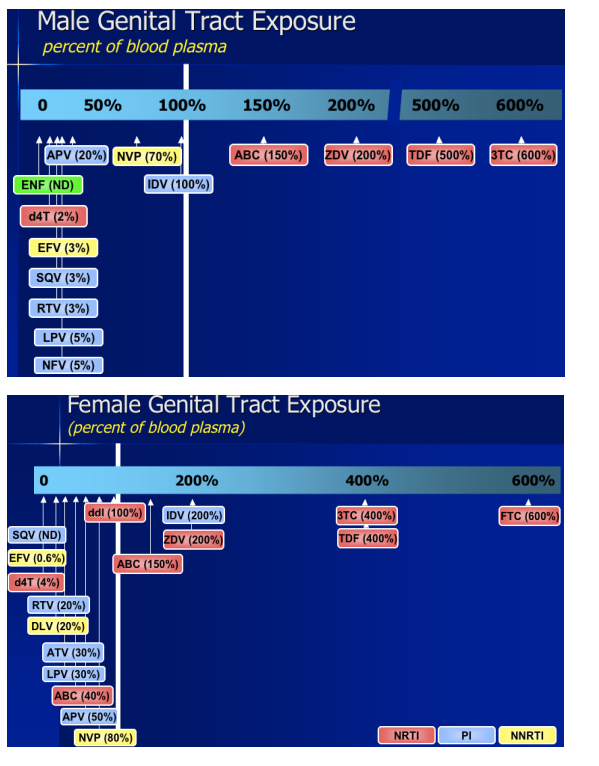
Conclusions: Understanding exposure profiles for ARVs in the GT is particularly important for PREP, PEP, and possibly the prevention of mother-to-child-transmission. ZDV, 3TC, and FTC achieve GT exposures greater than that of BP. Since standard BP CONC for these agents have demonstrated virologic efficacy, it would be expected that the higher GT CONC would make these excellent candidates for PREP/PEP regimens. ATV and ddI achieve moderate GT CONC and may also prove useful in these regimens (ATV in particular with a low IC50 for HIVWT). ARVs achieving <10% of BP exposure in the GT (d4T, LPV, EFV) may be less optimal candidates.
From day 1 to steady state, TFV exposures were high in the genital tract of men (extra- and intracellular) and women (extracelluar)
"A Pharmacologic Basis for the Use of Tenofovir In Pre- and Post-exposure Prophylaxis: Intra- and Extracellular Genital Tract Pharmacokinetics and Pharmacodynamics from First Dose to Steady State in HIV-1-infected Men and Women"
Manoli Vourvahis*1, H Tappouni1, K Patterson1, Y C Chen1, N Rezk1, S Fiscus1, B Kearney2, J Rooney2, M Cohen1, and A Kashuba1
1Univ of North Carolina at Chapel Hill, US and 2Gilead Sci, Foster City, CA, US
Background: Tenofovir (TFV) is effective in preventing HIV transmission in animal models, and is being investigated for pre-exposure prophylaxis in a number of populations. However, no comprehensive data exist describing TFV exposure in the genital tract. This is the first study to measure TFV extracellular and intracellular diphosphate (TFV-DP) concentrations in the genital tract of men and women from day 1 to steady-state.
Methods: A non-blinded pharmacokinetic study was performed in HIV-1-infected subjects (9 men, 13 women). A subset (8 men, 1 woman) underwent 14-day monotherapy to assess TFV effects on genital tract HIV-1 RNA. For men, paired blood and genital tract samples were obtained 24 hours post-dose on day 1, 3, 5, and 7. At steady state (≥14 days), 10 blood and 5 genital tract samples were obtained over 24 hours. For women, 6 paired blood and genital tract samples were obtained over 24 hours on day 1 and at steady state. Intracellular concentrations were measured in mononuclear cells isolated from blood, semen, and cervical cytobrush samples using percoll or Dynabeads. Genital tract extracellular concentrations were measured in blood, plasma, seminal plasma, or directly aspirated cervicovaginal fluid. Concentrations were measured by validated LC/MS/MS and LC/UV assays. Blood and genital tract HIV-1 RNA were measured by Roche Amplicor HIV-1 Monitor UltraSensitive and Nucli-Sens HIV-1 kits. Data were analyzed using noncompartmental pharmacokinetic and nonparametric statistical methods. Data are presented as mean (SD).
Results: At 24 hours, intracellular TFV-DP genital tract-to-blood ratios in men for day 1 and 7 were 3.1±5.4 and 7.0±14.8, respectively. TFV-DP could not be detected in the genital tract of all women and some men due to low cell yields (<106 cells/sample). TFV exposures were significantly greater (p <0.05) in genital tract than blood at both day 1 and steady state in men and women. Over 14 days in men, HIV-1 RNA decreased by 1.1±0.5 log10 copies/mL in blood and 1.0±0.4 log10 copies/mL in genital tract (p <0.05). In the 1 woman on TFV monotherapy, HIV-1 RNA decreased by 0.8 log10 copies/mL in both blood and genital tract.
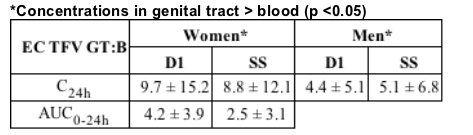
Conclusions: From day 1 to steady state, TFV exposures were high in the genital tract of men (extra- and intracellular) and women (extracelluar). These extra- and intracellular genital tract exposures are the highest (relative to blood) among other ART reported to date. TDF monotherapy significantly reduced both blood and genital tract HIV-1 RNA over 14 days. The rapid achievement of high extra- and intracellular concentrations in the genital tract of men and women is encouraging, and supports further study of TDF in pre- and post-exposure prophylaxis trials.
|
|
| |
| |
|
|
|
|
|