 |
|
|
| |
Pharmacokinetics (PK) and antiretroviral (ARV) response to TMC114/r and TMC 125
combination in patients with high level viral resistance
|
| |
| |
Reported by Jules Levin
13th CROI, Feb 5-8, 2006
authors: Marta Boffito1, Alan Winston1, Carl Fletcher1, Anton Pozniak1, Mark Nelson1, Graeme Moyle1, Izabela Tolowinska1, Richard
Hoetelmans2, Diego Miralles2, Brian Gazzard1
1 St Stephen's Centre, C&W Hospital, London, UK. 2 Tibotec BVBA, Mechelen, Belgium.
The purpose of this study was to investigate the pharmacokinetics,
efficacy, safety and tolerability of the co-administration of TMC125 plus
TMC114 with low-dose RTV in multi-experienced HIV-infected subjects
with limited therapeutic options; average 75 CD4s, 4 primary PI mutations, 7 NRTI mutations, 2 NNRTI mutations.
Following screening procedures (days -14 to -1), all subjects commenced
on day 1. TMC125 (200 mg bid) and TMC114/RTV (600/100 mg bid)
together with two or more NRTIs, plus or minus enfuvirtide (ENF).
On days 7 and 28, subjects were administered TMC125 plus TMC114/RTV
in the Unit within 15 min of completing a standardized meal. Serial blood
samples for PK assessment were collected over a period of 12 h: 0 (10 min
before dosing), 0.5, 1, 1.5, 2, 3, 4, 6, 9, 12 h post dose.
PK Analysis:
Plasma PK parameters [area under the curve from 0 to 12 hours
(AUC12h), maximum concentration (Cmax), pre-dose concentration (C0h)
and minimum concentration (Cmin)] for TMC125 and TMC114 were
calculated using non-compartmental methods utilizing a PK data
analysis program (WinNonLin version 4.01a). The AUC was calculated
using linear/log trapezoidal rule.
TMC125 and TMC 114 PKs was compared with historical data obtained
from subjects on TMC125 in the absence of TMC114 and TMC114 in
the absence of TMC125.
RESULTS
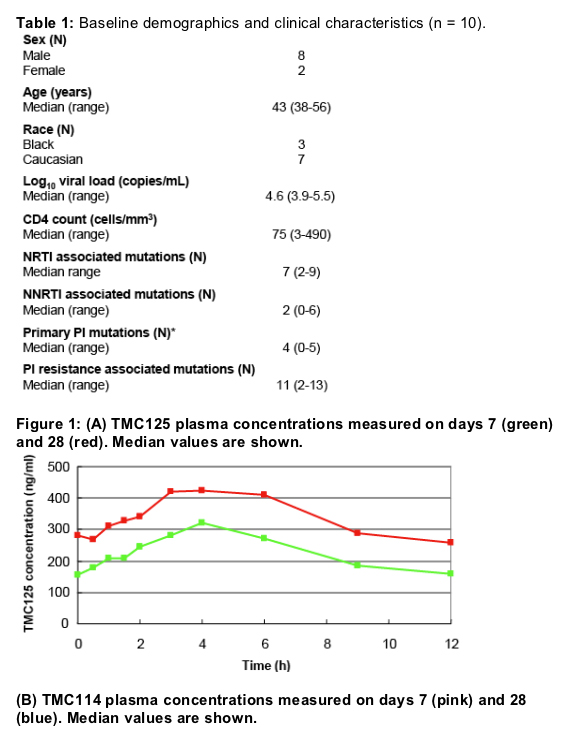
Ten/11 patients completed both PK phases; baseline demographic and
clinical characteristics are summarised in Table 1.
All patients had viruses with high level PI resistance (Table 1 and 2).
Six/10 patients had prior exposure to tipranavir (TPV) and to ENF; only 2
used ENF for the first time (Table 2).
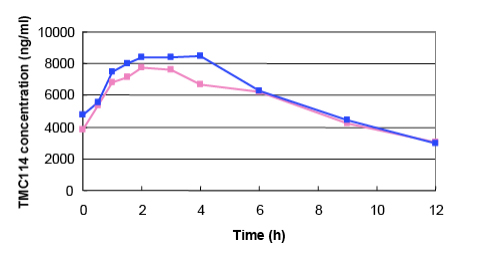
The PKs of TMC125 and TMC114 measured on days 7 and 28 is
illustrated in Table 3 and Figure 1.
As compared to historical controls, these reflect modestly reduced
(30%) exposure to TMC125. However, values for TMC125 PK are
similar to those previously measured when co-administering TMC125
with a boosted PI (median TMC125 AUC and C0h from historical data:
3556 and 196).
Exposure to TMC114 was similar to previously measured values
measured in the absence of TMC125.
Coefficient of variation (CV) in TMC125 and TMC114 PK parameters
ranged from 27 to 70% (Table 3).
At week 12, all patients had achieved at least a 2 log10 decrease in HIVRNA
with a median of -2.76; all subjects had a VL < 400 copies/mL (8 <
40 copies/mL) (Table 2 and Figure 2).
Median (range) CD4 increase was 87 (83-171) cells/mm3 (Table 2 and
Figure 2).
No serious adverse events or changes in lab safety were reported.
Possibly drug related adverse events were: mild diarrhoea (n = 1),
headache (n = 1), grade 1 skin rash (n = 1), which all resolved with
continuous dosing.
No statistically significant associations were observed between log10
change in VL and TMC114 or TMC125 PK parameters, TMC114
inhibitory quotient (IQ) or use of ENF.
Authors concluded: No significant PK interaction between TMC125 and
TMC114 was observed. The combination was well tolerated and showed impressive short-term efficacy against three-class resistant HIV. Further studies of this combination are warranted.
BACKGROUND:
Resistance and cross-resistance to ARVs remain a major reason for treatment failure and exhaustion of therapeutic options1.
Development of new, potent and tolerable ARVs with improved resistance profiles is urgently needed for the growing number of subjects with multi-drug resistant HIV and otherwise limited treatment options.
Furthermore, it is expected that the administration of two or more susceptible ARVs in this patient population would lead to enhanced treatment efficacy and durability1.
TMC125 is a novel NNRTI designed to have a high genetic barrier to the
development of resistance2. In a 7-day trial, TMC125 monotherapy produced a mean change in viral load (VL) of - 0.9 log10 copies/mL in patients failing NNRTI-based therapy3 and phase II trials in triple-classexperienced patients found that TMC125 was generally safe and well tolerated and showed significant and sustained efficacy, suggesting that TMC125 is the first NNRTI to show significant activity in patients with prior NNRTI failure4. A new formulation of TMC125 is today available: 100 mg tablets with significantly improved bioavailability, dosage 200 mg bid showed a comparable exposure to 800 mg bid of previous formulation5.
TMC114 is a potent, new non-peptidic protease inhbitor (PI) that, in combination with low dose (ritonavir) RTV, has shown activity in naïve and experienced patients. In these patients, TMC114/RTV produced a rapid and robust VL reduction and was well tolerated6. Moreover, TMC114 has demonstrated long term efficacy in patients with PI resistance and has been filed for regulatory approval.
The drug interaction between TMC125 and TMC114 has not been
characterized in HIV-infected patients.
The purpose of this study was to investigate the pharmacokinetics,
efficacy, safety and tolerability of the co-administration of TMC125 and
TMC114 with low-dose RTV in multi-experienced HIV-infected subjects
with limited therapeutic options.
|
|
| |
| |
|
|
|
|
|