 |
|
|
| |
Lack of Effect of Acid Reducing Agents on the Pharmacokinetics (PK)
of Lopinavir/Ritonavir (LPV/r) Tablet Formulation
|
| |
| |
CE Klein, Y-L Chiu, Y Cai, K Beck, KR King, SJ Causemaker, TT Doan, HU Esslinger, TJ Podsadecki, and GJ Hanna;
Abbott Laboratories, Abbott Park, IL, USA; Abbot GmBH, Ludwigshafen, Germany
Study objective:
To determine the effect of a proton-pump inhibitor (OME) and an H2 antagonist (RAN) on the PK of LPV/r tablet administered QD or BID and ATV+ RTV dosed QD.
ABSTRACT
Background: Acid reducing agents, including proton pump inhibitors (e.g. omeprazole, OME) and H2 antagonists (e.g. ranitidine, RAN), are used extensively by HIV-infected patients and decrease bioavailability of some antiretroviral agents. The effect of acid reducing agents on LPV/r in any formulation has not been formally assessed, and the influence of
decreased stomach acidity on drug bioavailability from a novel melt-extrusion LPV/r tablet is unknown. We determined the effect of OME and RAN on the PK of LPV/r tablet administered once or twice daily (QD or BID) and atazanavir (ATV) boosted by ritonavir (RTV) capsule.
Methods: 71 healthy (HIV-negative) adults were randomized to receive LPV/r tablets 400/100 mg BID or 800/200 mg QD or RTV capsule 100 mg + ATV 300 mg QD from Study Days 1 to 15 approximately 30 minutes after a meal. Either OME 40 mg QD was administered 1 hour before breakfast on Study Days 11 to 15 or RAN 150 mg was administered 1 hour before breakfast on Study Day 11. Serial blood samples were collected during a dosing interval (for 12 or 24 hours after dosing) on Study Days 10, 11, and 15. The PK parameters of lopinavir
(LPV), RTV and ATV were compared with and without OME or RAN using point estimates and 90% confidence intervals.
Results: The comparison of LPV and RTV PK with and without OME or RAN for LPV/r is shown below.
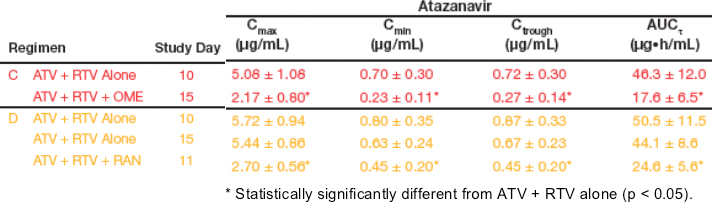
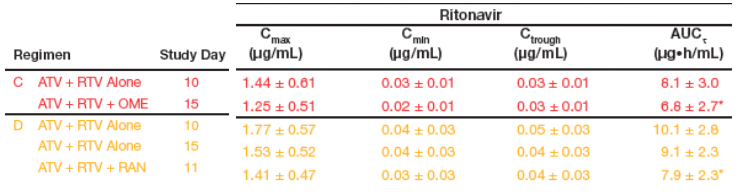
As previously shown, ATV levels were significantly decreased but RTV levels were unchanged with administration of ATV + RTV with OME or RAN.
Conclusions: Acid reducing agents do not significantly alter LPV or RTV exposure after co-administration with LPV/r 400/100 mg BID or 800/200 mg QD or with RTV 100 mg QD. Drug bioavailability from a novel melt-extrusion LPV/r tablet is not altered by acid reducing agents.
INTRODUCTION
Protease inhibitors have shown various degrees of interaction with acid reducing agents, including proton pump inhibitors and H2 antagonists, according to their dependency on pH for adequate solubility.
- ATV bioavailability has been shown to be decreased by 14 to 94% with acid reducing agents.1
- Fosamprenavir bioavailability has been shown to be decreased by 18 to 30% with acid reducing agents.2
- Saquinavir bioavailability has been shown to be increased by 82 to 120% with acid reducing agents.3
- Indinavir bioavailability has been shown to be unchanged to 47% lower with acid reducing agents.4
Acid reducing agents are used extensively by HIV-1 infected patients and the influence on the bioavailability of LPV/r has not been definitively assessed.
- LPV solubility is not dependent on pH.
- The solubility of RTV decreases slightly at pH >3.
- A retrospective analysis of HIV-1 infected subjects suggested no difference in LPV trough concentrations (Ctrough) when LPV/r soft gelatin capsule (SGC) was
co-administered with acid reducing agents.5
A new tablet formulation of LPV/r was recently approved in the United States which decreases the daily pill count from 6 SGCs to 4 tablets, eliminates the need for refrigeration, and allows administration without regard to meals.6
STUDY METHODS & DESIGN
Healthy HIV-negative adults (N=71) were enrolled into this multiple-dose, non-fasting, open-label, parallel-arm drug interaction study if they met the following criteria:
- General good health
- No concomitant medication
- Body mass index was between 18 and 29 kg/m2.
Each protease inhibitor (LPV/r and ATV + RTV) was administered following a moderate-fat meal (20-30% from fat), as ATV is currently recommended to be taken with food.
Each acid reducing agent (RAN and OME) was administered after a 7.5-hour fast and 1.5 hours prior to protease inhibitor dosing to maximize the pH during the absorption of LPV/r, ATV, and RTV.
- As proton pump inhibitors require chronic administration for maximal efficacy, OME was administered for 5 days.
- Due to the potential for tolerance with H2 antagonists, and to reflect intermittent use patterns in patients taking RAN on an as-needed basis, RAN was administered only for one day.
REGIMENS That included OME:
Regimen A: LPV/r 400/100 mg bid
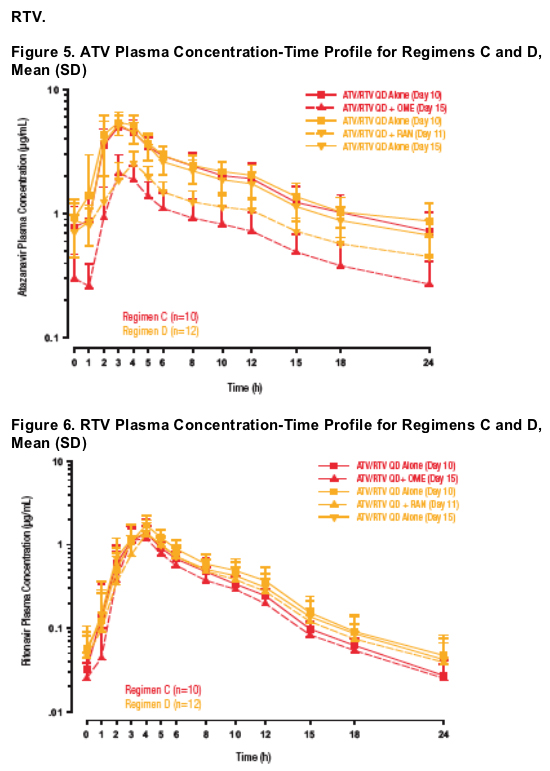
Regimen C; ATV+RTV 300/100 mg QD
Regimen E: LPV/r 800/200 mg QD
REGIMENS That included RAN:
Regimen B: LPV/r 400/100 mg bid
Regimen D: ATV+RTV 300/100 mg QD
Regimen F: LPV/r 800/200 mg QD
On day 10 intensive PK sampling was conducted for regimens A, C & E. And on day 11 40 mg OME QD was added to each regimen, and intensive PK sampling was done on day 15. On day 10 & 11 intensive PK sampling was done for regimens B, D, and F, when 150 mg RAN was added. Intensive PK sampling was done on day 15.
Pharmacokinetic Analysis
Blood samples for this analysis were collected during a dosing interval for LPV, RTV and ATV assay on Study Day 10, Study Day 11 (Regimens B, D, and F only), and on Study Day 15.
A single blood sample was collected at the time of protease inhibitor dosing on Study Day 11 for RAN assay (Regimens B, D, and F only) and on Study Day 15 for OME assay
(Regimens A, C, and E only).
Drug concentrations for LPV, RTV, ATV and OME were measured by validated HPLC/MS/MS methods:
- LPV lower limit of quantitation (LLOQ) = 19.38 ng/mL
- RTV LLOQ = 11.07 ng/mL
- ATV LLOQ = 4.76 ng/mL
- OME LLOQ = 1.00 ng/mL
Drug concentrations for RAN were measured by a validated HPLC ultraviolet detection method:
- RAN LLOQ = 10.0 ng/mL
LPV, RTV and ATV PK parameters were calculated with standard non-compartmental analysis using WINNONLIN v. 5.1 software (Pharsight Corp., Mountain View, CA) to estimate the maximum observed concentration (Cmax), minimum observed concentration (Cmin), Ctrough, and area under the plasma concentration time curve during a dosing interval (AUCt), including the AUC from time 0 to 12 hours after dosing (AUC12) for BID regimens and the AUC from time 0 to 24 hours after dosing (AUC24) for QD regimens.
Statistical Analysis
A paired t-test was performed for Tmax and the logarithms of Cmax, AUC, Cmin and Ctrough for each of LPV, ATV and RTV, to compare the difference between Study Day 10 (without OME or RAN) and Study Day 11 (with RAN ) or Study Day 15 (with OME). Within the paired t-test analysis framework on the logarithms of Cmax, AUC and Ctrough, the bioavailability for Study
Day 11 or 15 relative to that of Study Day 10 was assessed. In addition, a mixed linear model, which contained a repeated effect, was used to compare the difference between Study Days 10 and 15 (without RAN) and Study Day 11 (with RAN). This model used all of the available data and provides a more robust measure of the effect of RAN on LPV/r or ATV + RTV.
Safety Analysis
Safety and tolerability were assessed throughout the study based on reported adverse events, vital signs and clinical laboratory measurements.
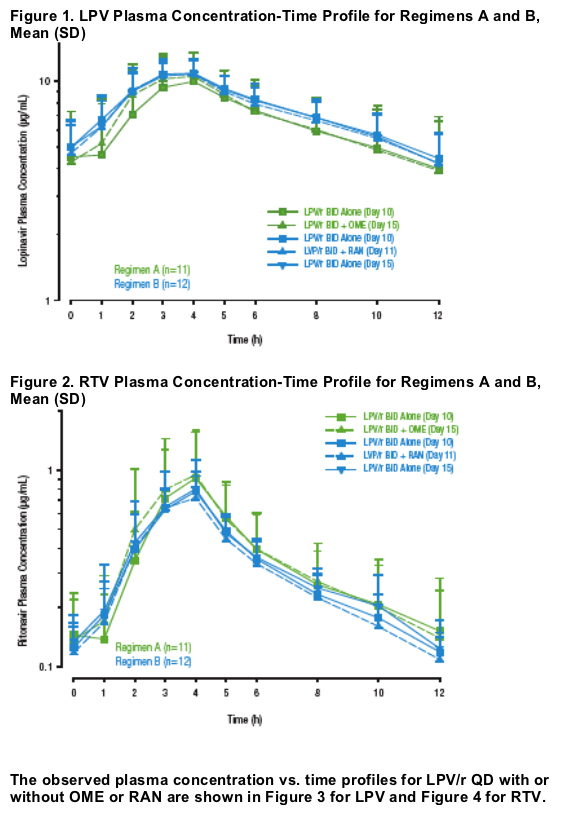
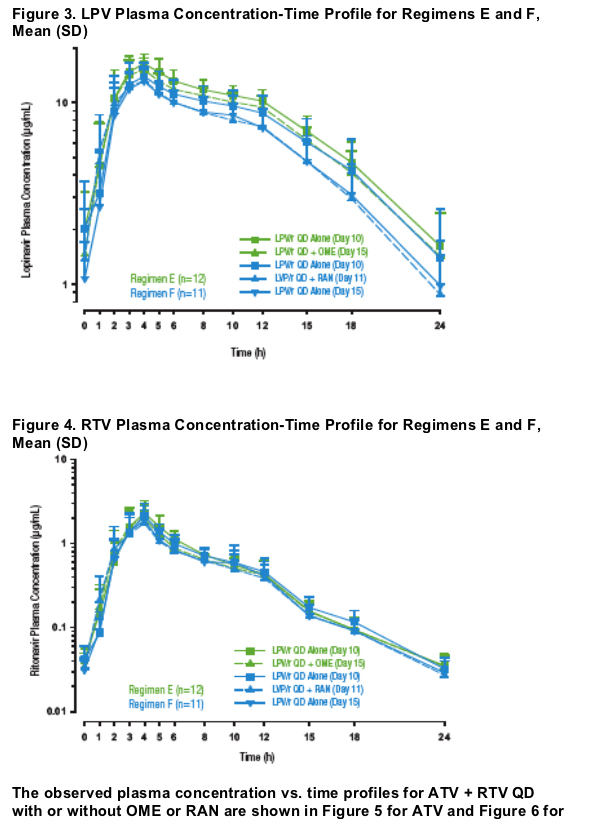
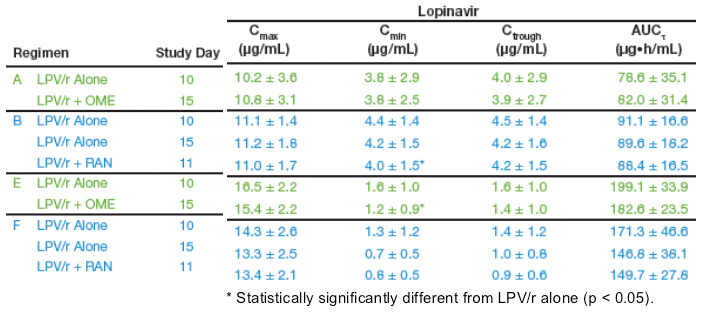
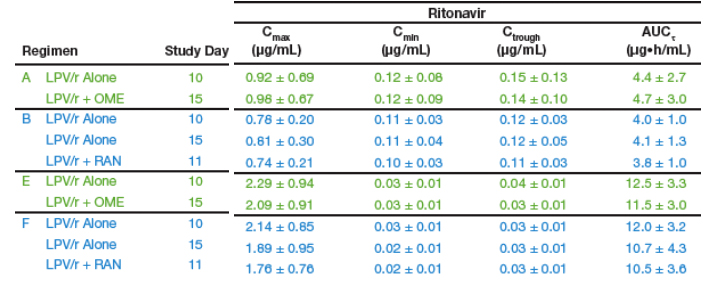
When comparing the pharmacokinetics of LPV/r 400/100 mg BID tablet or 800/200 mg QD tablet with and without OME or RAN:
- The point estimates for LPV and RTV were close to 1.0, suggesting that LPV/r bioavailability is not influenced by acid reducing agents.
When comparing the pharmacokinetics of ATV + RTV 300 + 100 mg QD with and without OME or RAN:
- ATV Cmax and AUC12 were decreased by 48 to 62%.
- The point estimates for RTV Cmax and AUC12 were similar to what was seen with LPV/r tablet.
A mixed-model analysis was used to take advantage of the additional data on Study Day 15 for Regimens B, D, and F. This is a more robust measure of the effect of RAN on LPV/r or ATV + RTV. The comparison of PK with and without RAN is shown in Table 5.
It was noted that one subject significantly contributed to the point estimates and 90% confidence intervals for Regimen F. This individual had high drug exposure on Study Day 10, average exposure on Study Day 11, and below average exposure on Study Day 15. If this subject is excluded from the paired t-test the results are consistent with those seen from the mixed effects model.
Concentrations of OME and RAN at the time of protease inhibitor dosing are shown in Table 6.
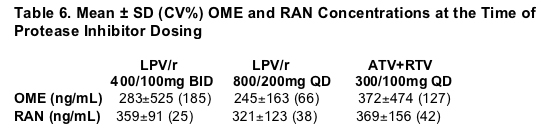
The concentrations of OME are within the Cmax and Cmin reported in studies of 40 mg OME QD. The concentrations of RAN are similar to those previously reported for Cmax following a 150 mg dose.
|
|
| |
| |
|
|
|
|
|