| |
The Maze of Treatments for Hepatitis B
|
| |
| |
New England Journal of Medicine
June 30, 2005
Anna Suk-Fong Lok, M.D.
>From the Division of Gastroenterology, University of Michigan Medical Center, Ann Arbor.
Worldwide, there are approximately 350 million carriers of hepatitis B virus (HBV), of whom half a million to 1 million die from liver disease each year. The goal of treatment for chronic hepatitis B is to prevent cirrhosis, hepatic failure, and hepatocellular carcinoma. This goal is best achieved by eradicating HBV before irreversible liver damage occurs. However, the eradication of HBV is impossible to achieve because of the presence of extrahepatic reservoirs of HBV, the integration of HBV DNA into the host genome, and the presence of an intracellular conversion pathway that replenishes the pool of transcriptional templates (covalently closed circular HBV DNA) in the hepatocyte nucleus without the need for reinfection. Thus, withdrawal of treatment is usually accompanied by rapid viral rebound.
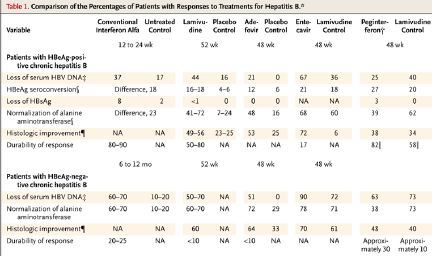
Currently, there are five approved therapies for chronic hepatitis B in the United States - interferon alfa-2b, lamivudine, adefovir, entecavir, and pegylated interferon (peginterferon) alfa-2a. Table 1 shows a comparison of the efficacy of these treatments.1,2 To approve treatments for hepatitis B, the FDA and other regulatory authorities use criteria that are based on responses after one year of treatment. However, very few patients will have a sustained response after one year of treatment. The benefits versus the risks of long-term treatment of chronic hepatitis B have not been properly studied. Given the variable natural course of HBV infection and the high costs of treatments ($5,000 to $15,000 a year, in U.S. dollars), decisions regarding whom to treat and with what and for how long must be carefully weighed.
In their study in this issue of the Journal, Lau et al. report that a combination of peginterferon alfa-2a and lamivudine was associated with the greatest degree of virus suppression, followed by lamivudine monotherapy and peginterferon alone.3 However, the rates of hepatitis B e antigen (HBeAg) seroconversion at the end of 48 weeks of treatment were similar among the three groups.
Unlike lamivudine and other nucleoside or nucleotide analogues, interferon has immune modulatory as well as antiviral effects. Previous studies involving three-to-six-month courses of conventional interferon showed that HBeAg seroconversion frequently occurred a few months after cessation of treatment, presumably because of the lag between immune priming and the decrease in the expression of viral proteins. The study by Lau et al. used a longer duration of peginterferon therapy; nonetheless, a small increment in the rate of HBeAg seroconversion was observed after treatment was stopped, so that at week 72, the two groups that received peginterferon had significantly higher rates of HBeAg seroconversion than the group that received lamivudine monotherapy.
The study reported by Hadziyannis et al. in this issue of the Journal showed the results at week 96 and week 144 of a phase 3 clinical trial of adefovir dipivoxil in patients with HBeAg-negative chronic hepatitis B.6 An earlier report on this trial showed that at week 48, adefovir was associated with significantly higher rates of virologic, biochemical, and histologic responses than was placebo.4 The study by Hadziyannis et al. showed that these responses were negated in virtually all patients after treatment was stopped at week 48. These disappointing results confirm that current treatments suppress but do not eradicate HBV. They also highlight the inadequacies of the end points of trials used for the approval of treatments for HBV.
Among the patients who continued to receive adefovir from week 49 through week 96 or from week 97 through week 144, the rates of virologic response (defined as a serum HBV DNA level that was undetectable with the use of polymerase-chain-reaction assay) and biochemical response (normalization of levels of aminotransferases) were slightly higher than the rates after 48 weeks. However, 20 to 30 percent of the patients did not meet these criteria after 144 weeks of continuous therapy.
The main concerns with long-term treatment are side effects, drug resistance, and costs. Adefovir at high doses (≥30 mg per day) has been associated with nephrotoxicity.4 In the study by Hadziyannis et al., nephrotoxicity was observed in 3 of 70 patients who received adefovir for three years, necessitating discontinuation of the treatment in two patients. Unlike resistance to lamivudine, resistance to adefovir is considered to be uncommon and to emerge later in the course of treatment. In the current analysis, adefovir-resistance mutations were detected in 6 of 70 patients who received adefovir for three years.6 Thus, although response was maintained in most patients who continued treatment, nephrotoxicity and drug resistance will be of increasing concern with longer durations of treatment.
Ten years ago, conventional interferon was the only approved treatment for chronic hepatitis B. Since then, three orally administered nucleoside or nucleotide analogues and a long-acting (pegylated) interferon have been approved in the United States. Patients with chronic hepatitis B now have more treatment options that have fewer side effects and are more easily administered. This has broadened the indications for treatment for hepatitis B to include patients with decompensated HBV cirrhosis7 and patients who require HBV prophylaxis during chemotherapy for cancer.8 In addition, long-term treatment with lamivudine has been shown to decrease the risk of hepatic failure and hepatocellular carcinoma among patients with cirrhosis and high levels of HBV DNA.9
However, these new therapies have brought along new problems. Foremost is drug-resistance mutations.10 Selection of drug-resistance mutations is accompanied by virologic breakthrough (increased serum HBV DNA levels after initial suppression) and in some patients biochemical breakthrough (increased levels of aminotransferases after initial normalization) and, rarely, hepatic failure and death. In addition, resistance to one antiviral agent may confer resistance to other agents and may limit future treatment options. Another problem is the high rate of relapse when treatment is discontinued. Studies that compared peginterferon and lamivudine all showed a higher rate of virologic relapse when treatment with lamivudine was stopped.3,5,11 Although adefovir and entecavir have not been directly compared with interferon, existing data suggest that relapse is more common than with interferon.
Given multiple treatment options that are less than ideal, who should be treated, with what, and when can treatment be stopped? The decision to treat or not to treat and the choice of treatment should be made jointly by the physician and the patient and should balance the benefits and the risks (e.g., the likelihood of a sustained response after a defined course of treatment or a maintained response during long-term treatment vs. the risk of progressive liver disease, side effects, drug resistance, and costs). For HBeAg-positive patients, viral suppression without HBeAg clearance is invariably associated with relapse, whereas viral suppression with HBeAg clearance is associated with sustained responses in 50 to 90 percent of patients.1 For HBeAg-negative patients, relapse is frequent even when the virus has been suppressed to undetectable levels for more than a year.12 Patients who opt for interferon must be aware of the wide array of potential side effects, whereas those who opt for oral antiviral therapy must be aware of the need for long-term treatment and the risks of drug resistance.
For patients with HBeAg-positive chronic hepatitis B who do not yet have cirrhosis, the goal is to achieve HBeAg seroconversion. Because pretreatment aminotransferase levels are a strong predictor of HBeAg seroconversion (except in the study by Lau et al.),13 current guidelines do not recommend treatment of patients with normal aminotransferase levels unless liver biopsy shows substantial inflammation or fibrosis.1,14,15 For patients with HBeAg-negative chronic hepatitis B who do not yet have cirrhosis, a one-year course of treatment is associated with a 15 to 35 percent chance of sustained response after interferon therapy but a less than 10 percent chance after treatment with lamivudine or adefovir.1,6,10 Given the need for long-term treatment, current guidelines recommend treatment only for patients with elevated aminotransferase levels or histologic evidence of moderate or severe inflammation or advanced fibrosis.1,14,15 For patients with cirrhosis, the potential gains are higher. Treatment is recommended for patients with high HBV DNA levels, but it is unclear whether patients with low HBV DNA levels will derive the same benefits. It is also unknown whether treatment should be lifelong or whether clinical benefit can be maintained after several years of treatment. Given the propensity for HBV to persist, patients should be closely monitored when treatment is stopped, to avoid fatal flares.
Substantial progress has been made in treatments for hepatitis B in the past decade. However, finding an exit through the maze of new therapies remains a challenge, underscoring the need for careful deliberation before initiating treatment.
Dr. Lok reports having served as a paid consultant to and having received grant support from Roche, Gilead Sciences, GlaxoSmithKline, and Bristol-Myers Squibb.
References
1. Lok AS, McMahon BJ. Chronic hepatitis B: update of recommendations. Hepatology 2004;39:857-861. [CrossRef][ISI][Medline]
2. Entecavir Review Team. Briefing document for NDA 21-797, entecavir 0.5 and 1 mg tablets and NDA 21-798, entecavir oral solution 0.05 mg/mL. February 10, 2005 (memorandum). (Accessed June 9, 2005, at http://www.fda.gov/ohrms/dockets/ac/05/briefing/2005-4094B1_02_FDA-Background-Memo.pdf.)
3. Lau GKK, Piratvisuth T, Xian Luo K, et al. Peginterferon alfa-2a, lamivudine, and the combination for HBeAg-positive chronic hepatitis B. N Engl J Med 2005;352:2682-2695. [CrossRef]
4. Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al. Adefovir dipivoxil for the treatment of hepatitis B e antigen-negative chronic hepatitis B. N Engl J Med 2003;348:800-807. [Erratum, N Engl J Med 2003;348:1192.] [Abstract/Full Text]
5. Marcellin P, Lau GKK, Bonino F, et al. Peginterferon alfa-2a alone, lamivudine alone, and the two in combination in patients with HBeAg-negative chronic hepatitis B. N Engl J Med 2004;351:1206-1217. [Abstract/Full Text]
6. Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al. Long-term therapy with adefovir dipivoxil for HBeAg-negative chronic hepatitis B. N Engl J Med 2005;352:2673-2681. [CrossRef]
7. Fontana RJ, Hann HW, Perrillo RP, et al. Determinants of early mortality in patients with decompensated chronic hepatitis B treated with antiviral therapy. Gastroenterology 2002;123:719-727. [CrossRef][ISI][Medline]
8. Lau GK, Yiu HH, Fong DY, et al. Early is superior to deferred preemptive lamivudine therapy for hepatitis B patients undergoing chemotherapy. Gastroenterology 2003;125:1742-1749. [ISI][Medline]
9. Liaw Y-F, Sung JJY, Chow WC, et al. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med 2004;351:1521-1531. [Abstract/Full Text]
10. Fung SK, Lok AS. Management of hepatitis B patients with antiviral resistance. Antivir Ther 2004;9:1013-1026. [Medline]
11. Chan HL, Leung NW, Hui AY, et al. A randomized, controlled trial of combination therapy for chronic hepatitis B: comparing pegylated interferon-alpha2b and lamivudine with lamivudine alone. Ann Intern Med 2005;142:240-250. [Abstract/Full Text]
12. Fung SK, Wong F, Hussain M, Lok AS. Sustained response after a 2-year course of lamivudine treatment of hepatitis B e antigen-negative chronic hepatitis B. J Viral Hepat 2004;11:432-438. [CrossRef][ISI][Medline]
13. Perrillo RP, Lai CL, Liaw YF, et al. Predictors of HBeAg loss after lamivudine treatment for chronic hepatitis B. Hepatology 2002;36:186-194. [CrossRef][ISI][Medline]
14. de Franchis R, Hadengue A, Lau G, et al. EASL International Consensus Conference on Hepatitis B: 13-14 September, 2002 Geneva, Switzerland: consensus statement (long version). J Hepatol 2003;39:Suppl 1:S3-S25. [CrossRef][ISI][Medline]
15. Liaw YF, Leung N, Guan R, Lau GK, Merican I. Asian-Pacific consensus statement on the management of chronic hepatitis B: an update. J Gastroenterol Hepatol 2003;18:239-245. [CrossRef][ISI][Medline]
|
|
| |
| |
|
|
|