| |
Compromised CD4 Recovery in Treatment-Experienced Patients with HIV Receiving Both Tenofovir + ddI in the TORO Studies
|
| |
| |
Clinical Infectious Diseases Sept 15, 2005;41:901-905
Eugenia Negredo,1,2 Anna Bonjoch,1,2 Roger Paredes,1,2 Jordi Puig,1,2 and Bonaventura Clotet1,2
1Lluita contra la SIDA Foundation, Germans Trias i Pujol University Hospital, Badalona, and 2Universitat Autonoma de Barcelona, Barcelona, Spain
SUMMARY:
The effect of therapy with a combination of tenofovir and full-dose didanosine on increases in CD4+ cell count was examined in 2 large trials of treatment-experienced patients with human immunodeficiency virus (HIV) infection (the T-20 versus Optimized Regimen Only [TORO] 1 and 2 clinical trials). Individuals receiving both agents showed little additional increase in CD4+ cell count after week 8 of therapy, whereas those receiving 1 or neither of the agents had continuous increases over a 48-week period.
We have recently reported that HIV-infected patients receiving combinations containing both the nucleotide reverse-transcriptase inhibitor (NRTI) tenofovir disoproxil fumarate (TDF) (300 mg/day) and full dosages (400 mg/day in patients weighing >60 kg and a reduced dosage of 250 mg/day in patients weighing <60 kg) of the NRTI didanosine (ddI) experience unexpected decreases in CD4+ cell count, despite maintaining undetectable plasma viral loads [1]. At 48 weeks, >50% of the 302 patients in this study showed a decrease of >100 CD4+ cells/mm3, and up to 30% had a decrease of >200 cells/mm3. This finding is further supported by a recent retrospective analysis of patients with controlled viremia [2]. Patients receiving both ddI and TDF had a significant decline in CD4+ cell count over a 1-year treatment period, compared with those who took either drug alone or neither drug.
To investigate the effect of concomitant TDF and ddI therapy in a larger and more antiretroviral-experienced patient set, we examined changes from baseline in CD4+ cell count at week 48 of therapy in 2 phase III studies of the HIV-1 fusion inhibitor enfuvirtide (ENF) (TORO 1 & TORO 2, phase III studies for T20).
AUTHOR DISCUSSION:
Patients receiving TDF and full-dosage ddI treatment showed consistently poorer immune responses over a 48-week period in the TORO trials than did those patients receiving either 1 drug or neither of the drugs, even when adjusting for differences in baseline characteristics. The poorer responses observed were not associated with the degree of virologic suppression attained. The difference in immune response at week 48 only reached statistical significance in patients receiving a combination of ENF and OB (P = .045). However, the high degree of early treatment switching for virologic failure in the OB-only treatment arms of TORO (only 47% of patients who were initially receiving OB alone were still receiving OB alone at week 20) may have underestimated the difference between groups at week 48 in an ITT D/C=LOCF analysis of the OB-only and pooled treatment arms.
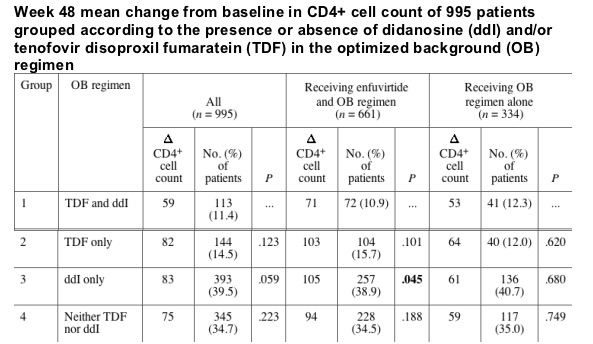
After adjusting for baseline prognostic factors (GSS, CD4+ cell count, HIV-1 RNA load, and number of positive prognostic factors), other antiretrovirals in the OB regimen, and randomization to ENF, group 1 consistently had the lowest gain in CD4+ cell count. This difference reached statistical significance between groups 1 and 3 in patients receiving a combination of ENF and OB.
The lower CD4+ cell response at week 48 in group 1, compared with the other groups, was not associated with having a virologic response. Overall, fewer patients in group 1 had undetectable viral loads (i.e., <400 copies/mL) at week 48 than in the other groups (19% vs. 27%-30% [ITT population], respectively). However, when only those patients with undetectable viral loads were considered (n = 269), the week 48 least squares mean change in CD4+ cell count was still lower in patients receiving a combination of ddI and TDF, compared with the other 3 groups (+119 vs. +164, +152, and +150 cells/mm3 for groups 1 vs. groups 2, 3, and 4, respectively; P = .279, .367, and .409, respectively]).
For patients receiving a combination of ENF and OB, continuous increases in CD4+ cell count over a 48-week period were noted in patients receiving either TDF or ddI. In contrast, patients receiving TDF and ddI together essentially ceased having increases in the CD4+ cell count after weeks 8-12. Similar results were noted for group 1 patients receiving OB alone.
Patients and methods.
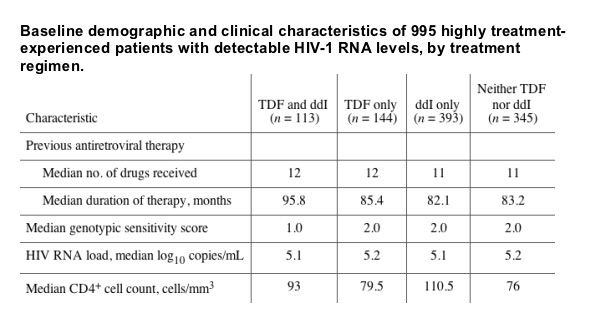
The T-20 versus Optimized Regimen Only (TORO) 1 and TORO 2 studies recruited highly treatment-experienced patients with detectable HIV-1 RNA loads who had received therapy for a mean duration of 7 years and had received a median of 12 previous antiretrovirals from all 3 conventional classes (NRTIs, nonnucleoside reverse-transcriptase inhibitors, and protease inhibitors) [3]. Patients were randomized 2 : 1 to receive treatment with ENF plus an optimized background (OB) of other antiretrovirals (selected on the basis of resistance testing) or treatment with an OB regimen without ENF. The genotypic susceptibility of virus to antiretrovirals was determined by the baseline genotypic sensitivity score (GSS), defined as the number of drugs in a patient's OB regimen to which their virus was genotypically susceptible. Positive prognostic factors have been identified that can predict outcomes of treatment with ENF [4]. These have been identified as baseline CD4+ cell count >100 cells/mm3, baseline HIV-1 RNA load <5 log10 copies/mL, prior treatment with <10 antiretrovirals, and >2 active antiretrovirals in the OB regimen (based on baseline phenotypic sensitivity score, defined as the number of drugs in a patient's OB regimen to which their virus is phenotypically sensitive).
Similar study designs and patient baseline characteristics allowed pooled analyses to be performed from a combined dataset of 995 patients. For the current analysis, patients from both the ENF plus OB arm and the OB only arm of the pooled TORO 1 and 2 trials were divided into 4 mutually exclusive treatment groups. Group 1 consisted of 113 patients with TDF and ddI in their OB regimen; 85% of these patients received a modal ddI dosage of 400 mg/day, 10% received a reduced modal dosage of 250 mg/day, and 5% received a modal dosage that was neither 400 nor 250 mg/day. Group 2 consisted of 144 patients receiving TDF without ddI. Group 3 consisted of 393 patients receiving ddI without TDF. Group 4 consisted of 345 patients receiving neither TDF nor ddI.
Changes from baseline in CD4+ cell count at week 48 of treatment were assessed using an analysis of covariance model for an intent-to-treat (ITT) population, with last observation carried forward for patients discontinuing randomized treatment (D/C=LOCF). Mean changes over time were assessed using observed data.
|
|
| |
| |
|
|
|